

National trends in open surgical, endovascular, and branched-fenestrated endovascular aortic aneurysm repair in Medicare patients
- PMID: 29290495
- PMCID: PMC5970963
- DOI: 10.1016/j.jvs.2017.09.046
National trends in open surgical, endovascular, and branched-fenestrated endovascular aortic aneurysm repair in Medicare patients
Abstract
Background: Open repair effectively prevents rupture for patients with abdominal aortic aneurysm (AAA) and is commonly studied as a metric reflecting hospital and surgeon expertise in cardiovascular care. However, given recent advances in endovascular aneurysm repair (EVAR), such as branched-fenestrated EVAR, it is unknown how commonly open surgical repair is still used in everyday practice.
Methods: We analyzed trends in open AAA repair, EVAR, and branched-fenestrated EVAR for AAA in Medicare beneficiaries from 2003 to 2013. We used Medicare Part B claims to ascertain counts of these repair types annually during the study period. We assessed regional and national trends in characteristics of the patients and procedure volume.
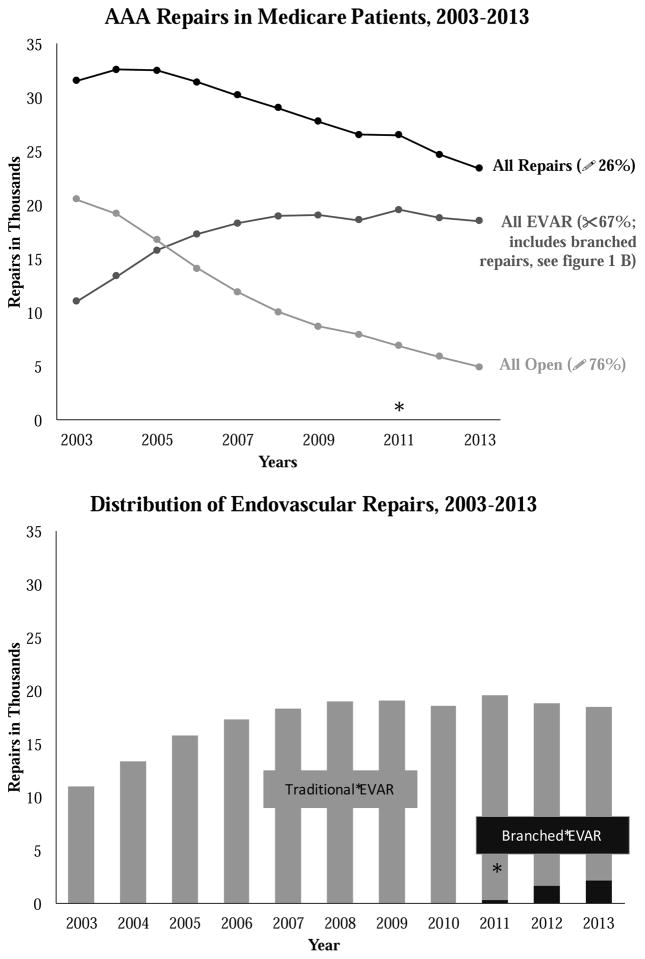
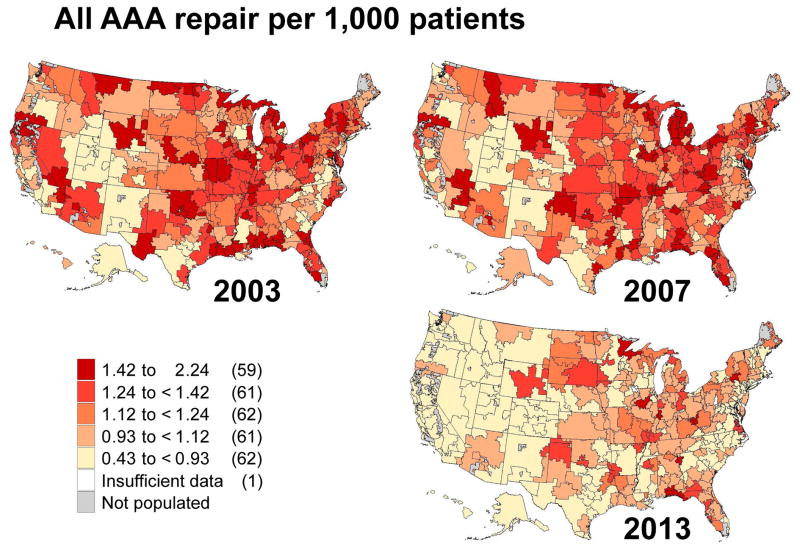
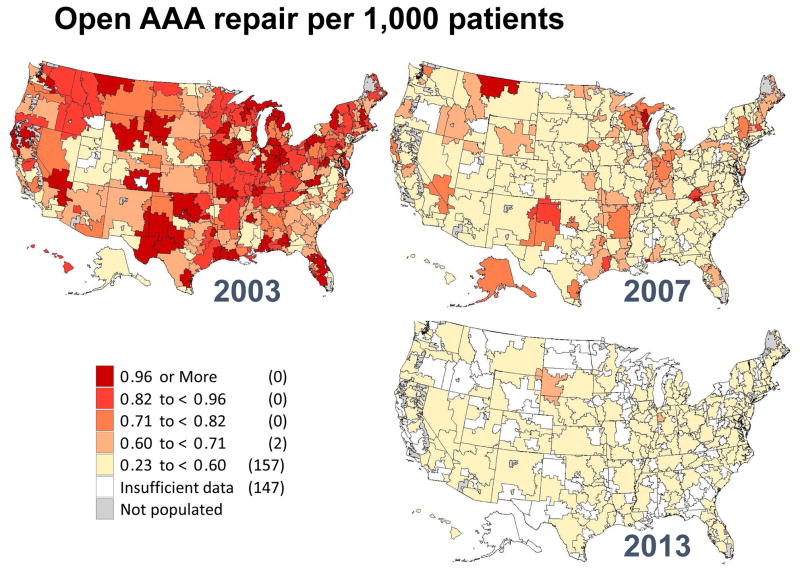
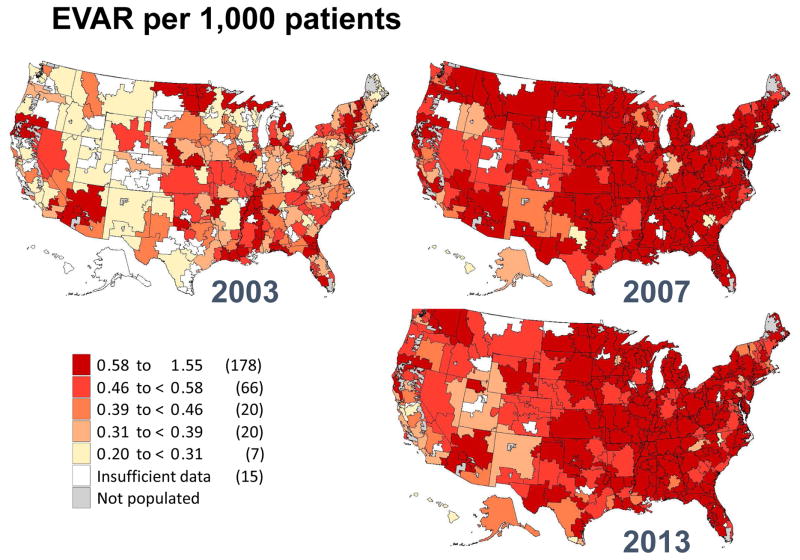
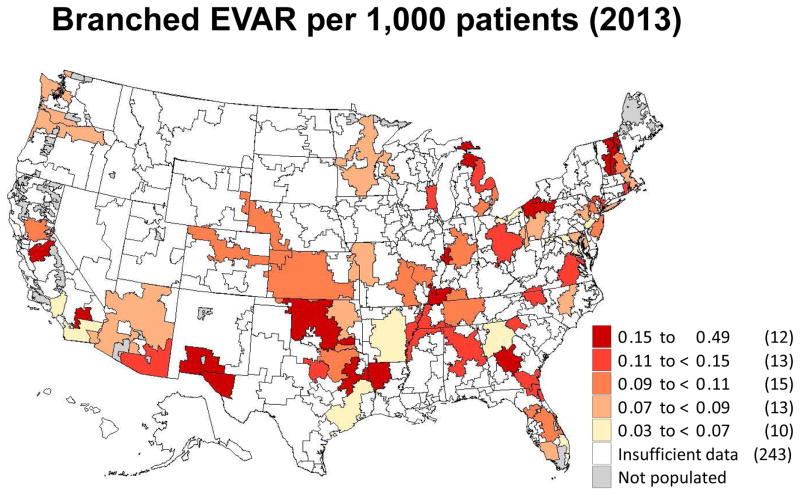
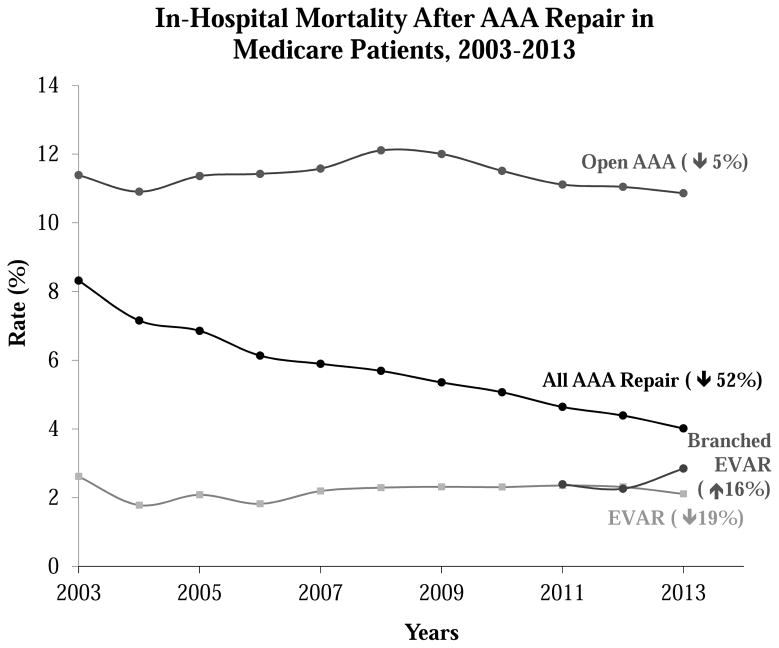
Results: Between 2003 and 2013, the total number of AAA repairs performed in fee-for-service Medicare patients declined by 26% from 31,582 to 23,421 (P < .001), after a peak number of 32,540 was performed in 2005 (28% decline since 2005). The number of open AAA repairs steadily declined by a total of 76%, from 20,533 in 2003 to 4916 in 2013 (P < .001). Whereas the number of EVARs increased from 11,049 in 2003 to 19,247 in 2011 (P < .001), it has since declined a total of 15% to only 16,362 repairs in 2013 (P < .001). After its introduction in 2011, the number of branched-fenestrated EVAR cases continuously rose from 335 procedures in 2011 to 2143 procedures in 2013 (P < .001). By 2013, virtually all hospital referral regions in the United States had rates of open AAA repair that would have been in the lowest quintile of volume in 2003.
Conclusions: The number of open AAA repairs fell by nearly 80% during the last decade, whereas traditional EVAR declined slightly and branched-fenestrated EVAR rapidly disseminated into national practice. These results suggest that open AAA repair is now performed too infrequently to be used as a metric in the assessment of hospital and surgeon quality in cardiovascular care. Furthermore, surgical training paradigms will need to reflect the changing dynamics necessary to ensure that surgeons and interventionists can safely perform these high-risk surgical procedures.
Copyright © 2017 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited commentary.J Vasc Surg. 2018 Jun;67(6):1698. doi: 10.1016/j.jvs.2017.10.060. J Vasc Surg. 2018. PMID: 29801552 No abstract available.
References
-
- Kurosawa K, Matsumura JS, Yamanouchi D. Current status of medical treatment for abdominal aortic aneurysm. Circ J. 2013;77(12):2860–6. - PubMed
-
- Agency for Healthcare Research and Quality. Abdominal aortic aneurysm (AAA) repair mortality: percentage of in-hospital deaths per 1,000 discharges with AAA repair, ages 18 years and older. 2015 [cited 2016 October 8th]; Available from: https://www.qualitymeasures.ahrq.gov/summaries/summary/49507?
-
- Dimick JB, Upchurch GR., Jr Measuring and improving the quality of care for abdominal aortic aneurysm surgery. Circulation. 2008;117(19):2534–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
