

Prolonged Dexmedetomidine Infusion and Drug Withdrawal In Critically Ill Children
- PMID: 29290746
- PMCID: PMC5736258
- DOI: 10.5863/1551-6776-22.6.453
Prolonged Dexmedetomidine Infusion and Drug Withdrawal In Critically Ill Children
Abstract
Objective: To characterise the incidence, symptoms and risk factors for withdrawal associated with prolonged dexmedetomidine infusion in paediatric critically ill patients.
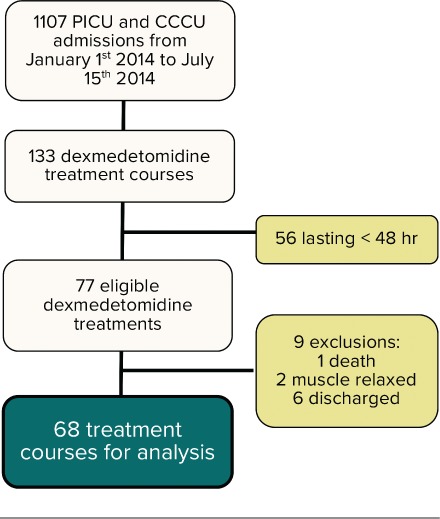
Methods: Retrospective chart review in the paediatric intensive care unit and the cardiac critical care unit of a single tertiary children's hospital. Patients up to 18 years old, who received dexmedetomidine for longer than 48 hours were included.
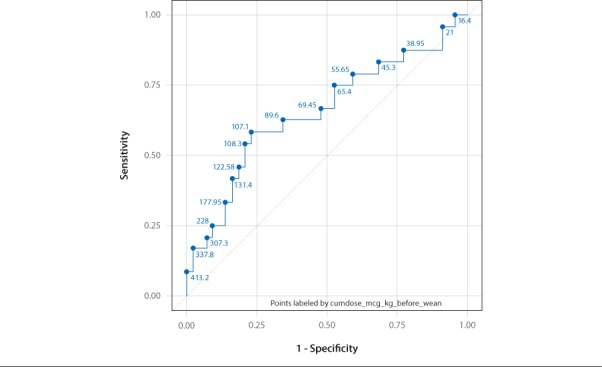
Results: A total of 52 patients accounted for 68 unique dexmedetomidine treatment courses of more than 48 hours. We identified 24 separate episodes of withdrawal in the 68 dexmedetomidine courses (incidence 35%). Of these episodes 38% occurred in patients who were weaned from dexmedetomidine alone while the remaining occurred in patients who had concurrent weans of opioids and/or benzodiazepines. Most common symptoms were agitation, fever, vomiting/retching, loose stools and decreased sleep. The symptoms occurred during the latter part of the wean or after discontinuation of dexmedetomidine. A cumulative dose of dexmedetomidine of 107 mcg/kg prior to initiation of wean was more likely associated with withdrawal (this equates to a dexmedetomidine infusion running at 1 mcg/kg/hr over 4 days). Duration of opioid use was an additional risk factor for withdrawal. The use of clonidine, as a transition from dexmedetomidine, did not protect against withdrawal (p = 1).
Conclusions: A withdrawal syndrome may occur after prolonged infusion of dexmedetomidine. As all our patients were also exposed to opioids this may be affected by the duration of opioid use. We identified a cumulative dose of 107 micrograms/kg of dexmedetomidine beyond which withdrawal symptoms were more likely (which equates to 4 days of use at a dose of 1 mcg/kg/hr). A protocol for weaning should be considered in this circumstance.
Keywords: dexmedetomidine; infusion; intensive care unit; intravenous; pediatric; substance withdrawal syndrome.
Conflict of interest statement
Disclosure The authors declare no conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria. The authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Figures
References
-
- Ista E, van Dijk M, Gamel C, . et al. Withdrawal symptoms in children after long-term administration of sedatives and/or analgesics: a literature review. “Assessment remains troublesome”. Intensive Care Med. 2007; 33 8: 1396– 1406. - PubMed
-
- Mason KP, Lerman J.. Review article: Dexmedetomidine in children: current knowledge and future applications. Anesth Analg. 2011; 113 5: 1129– 1142. - PubMed
-
- Tobias JD. Dexmedetomidine: applications in pediatric critical care and pediatric anesthesiology. Pediat Crit Care Med. 2007; 8 2: 115– 131. - PubMed
-
- Potts AL, Anderson BJ, Warman GR, . et al. Dexmedetomidine pharmacokinetics in pediatric intensive care--a pooled analysis. Paediatr Anaesth. 2009; 19 11: 1119– 1129. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials