

Unique metabolomic signature associated with hepatorenal dysfunction and mortality in cirrhosis
- PMID: 29291380
- PMCID: PMC6037419
- DOI: 10.1016/j.trsl.2017.12.002
Unique metabolomic signature associated with hepatorenal dysfunction and mortality in cirrhosis
Abstract
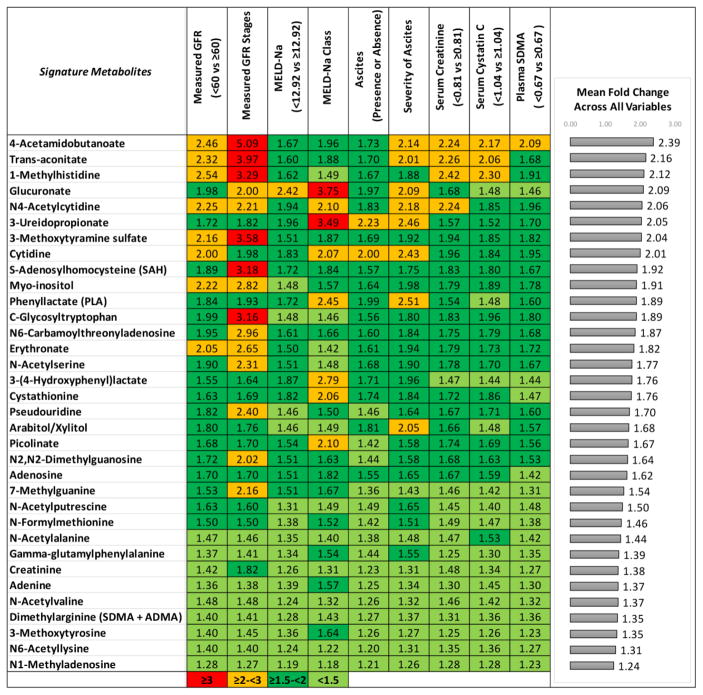
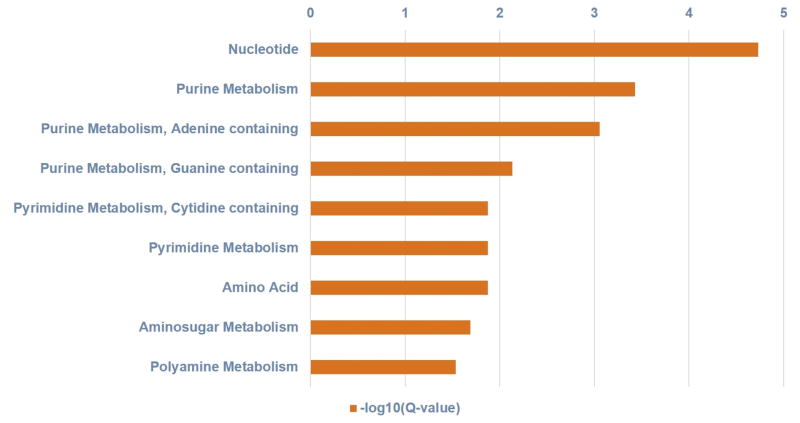
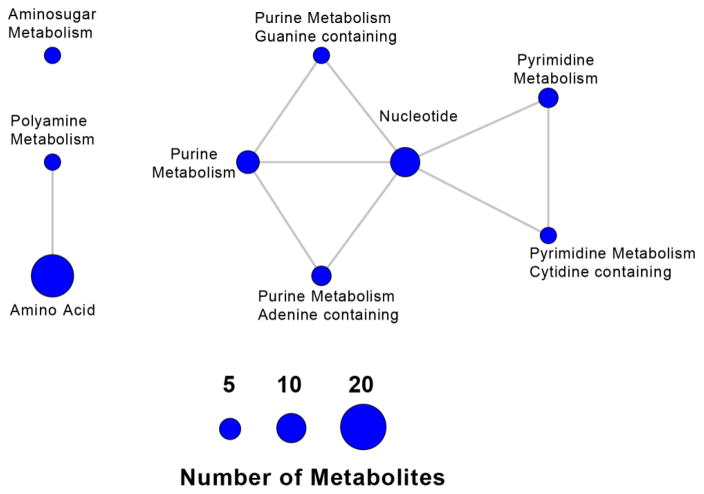
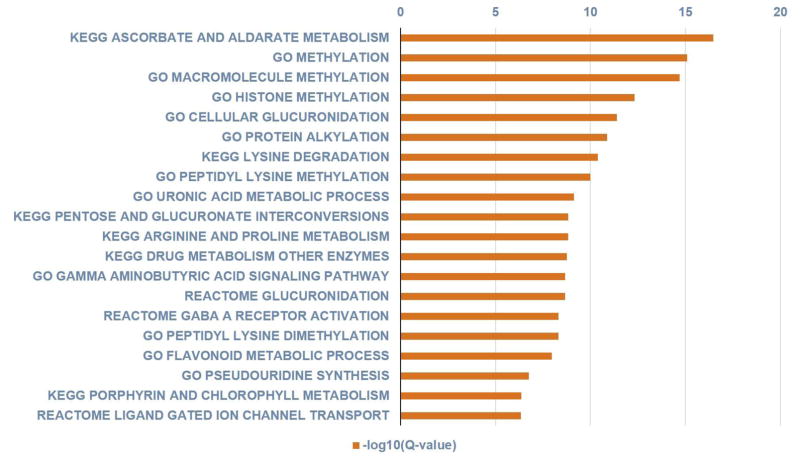
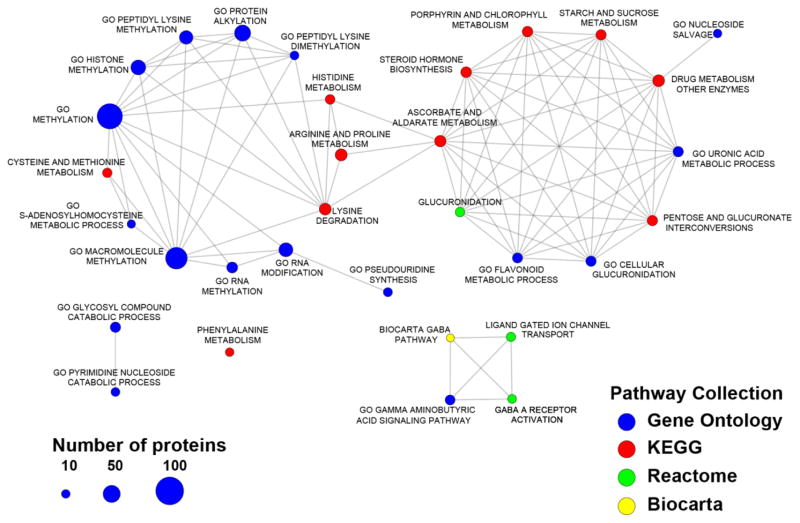
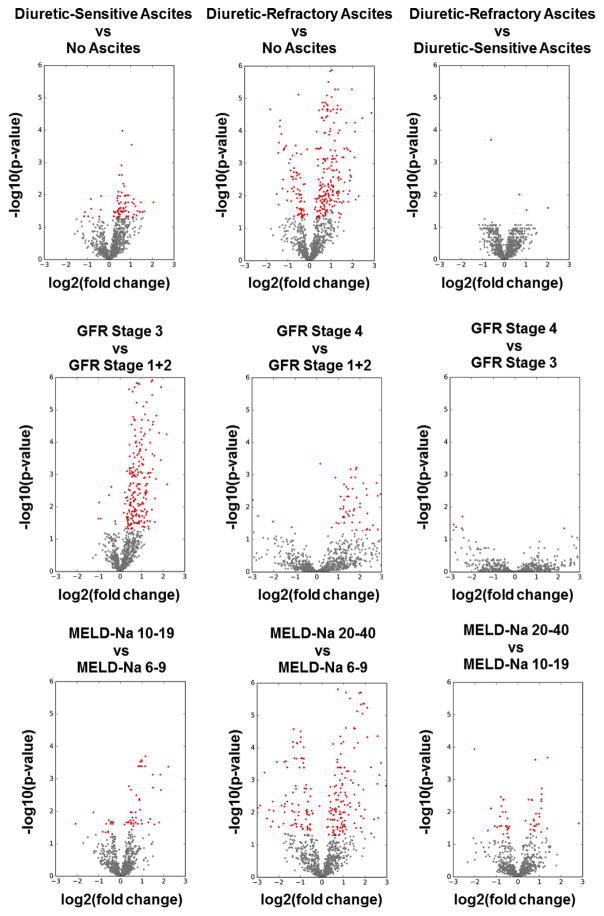
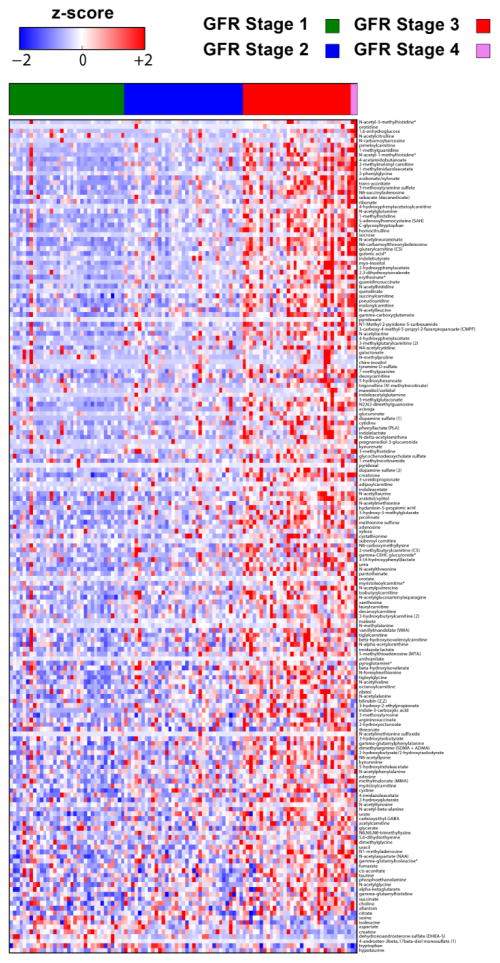
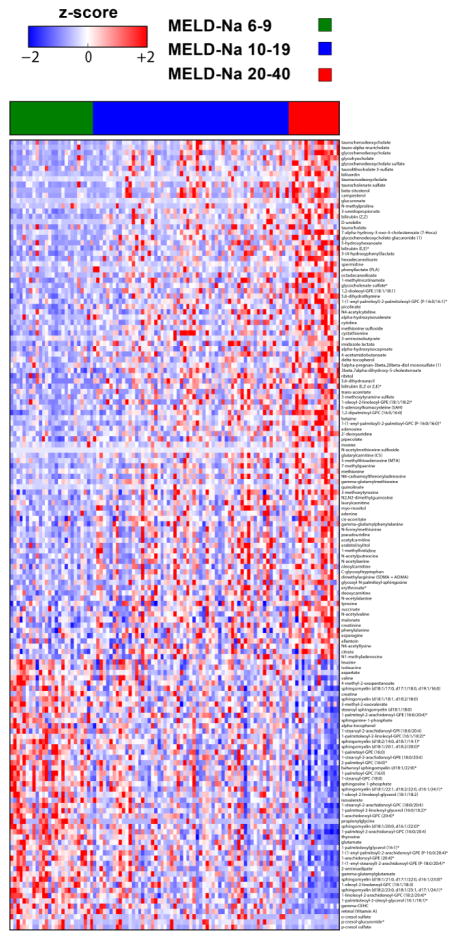
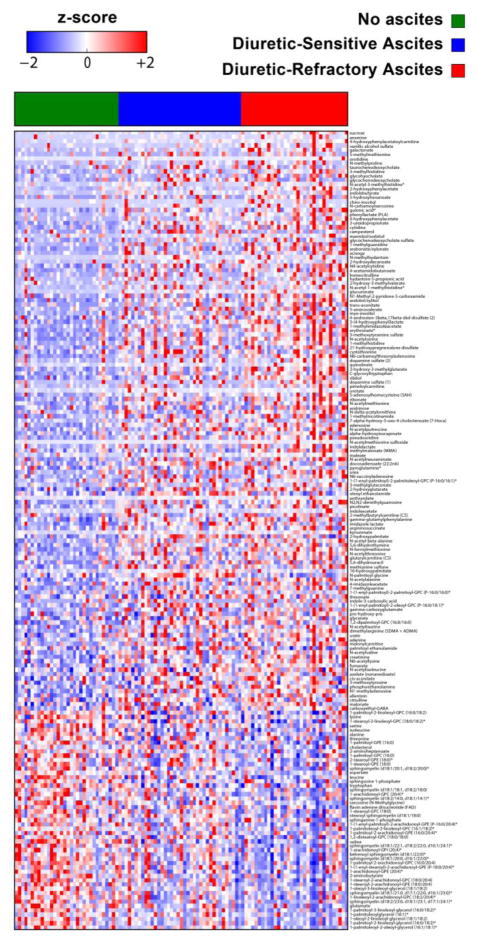
The application of nontargeted metabolomic profiling has recently become a powerful noninvasive tool to discover new clinical biomarkers. This study aimed to identify metabolic pathways that could be exploited for prognostic and therapeutic purposes in hepatorenal dysfunction in cirrhosis. One hundred three subjects with cirrhosis had glomerular filtration rate (GFR) measured using iothalamate plasma clearance, and were followed until death, transplantation, or the last encounter. Concomitantly, plasma metabolomic profiling was performed using ultrahigh performance liquid chromatography-tandem mass spectrometry to identify preliminary metabolomic biomarker candidates. Among the 1028 metabolites identified, 34 were significantly increased in subjects with high liver and kidney disease severity compared with those with low liver and kidney disease severity. The highest average fold-change (2.39) was for 4-acetamidobutanoate. Metabolite-based enriched pathways were significantly associated with the identified metabolomic signature (P values ranged from 2.07E-06 to 0.02919). Ascorbate and aldarate metabolism, methylation, and glucuronidation were among the most significant protein-based enriched pathways associated with this metabolomic signature (P values ranged from 1.09E-18 to 7.61E-05). Erythronate had the highest association with measured GFR (R-square = 0.571, P <0.0001). Erythronate (R = 0.594, P <0.0001) and N6-carbamoylthreonyladenosine (R = 0.591, P <0.0001) showed stronger associations with measured GFR compared with creatinine (R = 0.588, P <0.0001) even after controlling for age, gender, and race. The 5 most significant metabolites that predicted mortality independent of kidney disease and demographics were S-adenosylhomocysteine (P = 0.0003), glucuronate (P = 0.0006), trans-aconitate (P = 0.0018), 3-ureidopropionate (P = 0.0021), and 3-(4-hydroxyphenyl)lactate (P = 0.0047). A unique metabolomic signature associated with hepatorenal dysfunction in cirrhosis was identified for further investigations that provide potentially important mechanistic insights into cirrhosis-altered metabolism.
Published by Elsevier Inc.
Figures
References
-
- Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology. 2000;31(4):864–71. - PubMed
-
- Francoz C, Prie D, Abdelrazek W, Moreau R, Mandot A, Belghiti J, et al. Inaccuracies of creatinine and creatinine-based equations in candidates for liver transplantation with low creatinine: impact on the model for end-stage liver disease score. Liver Transpl. 2010;16(10):1169–77. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
