

Impact of an integrated care program on glycemic control and cardiovascular risk factors in patients with type 2 diabetes in Saudi Arabia: an interventional parallel-group controlled study
- PMID: 29291706
- PMCID: PMC5748946
- DOI: 10.1186/s12875-017-0677-2
Impact of an integrated care program on glycemic control and cardiovascular risk factors in patients with type 2 diabetes in Saudi Arabia: an interventional parallel-group controlled study
Abstract
Background: Long intervals between patient visits and limited time with patients can result in clinical inertia and suboptimal achievement of treatment goals. These obstacles can be improved with a multidisciplinary care program. The present study aimed to assess the impact of such a program on glycemic control and cardiovascular risk factors.
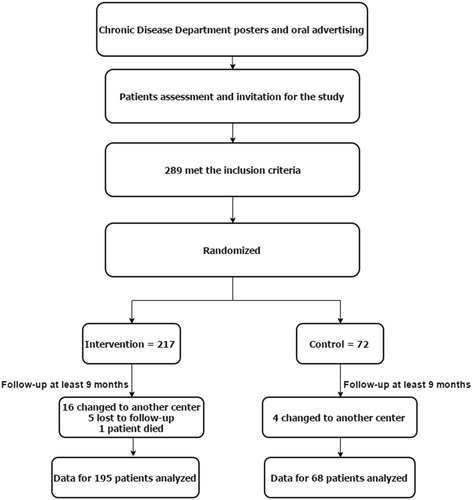
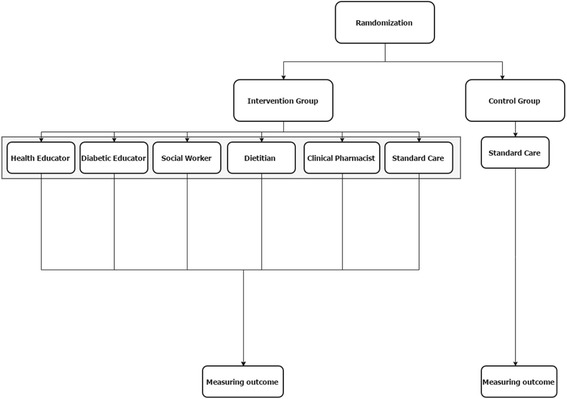
Methods: In a randomized, parallel-group trial, we assigned 263 patients with poorly controlled type 2 diabetes mellitus (T2DM) to either a control group, standard care program, or a multidisciplinary care program involving a senior family physician, clinical pharmacy specialist, dietician, diabetic educator, health educator, and social worker. The participants were followed for a median of 10 months, between September 2013 and September 2014. Glycated hemoglobin (HbA1c), fasting blood glucose (FBG), lipid profiles, and blood pressure (BP) were measured. The assignment was blinded for the assessors of the study outcomes. The study registry number is.
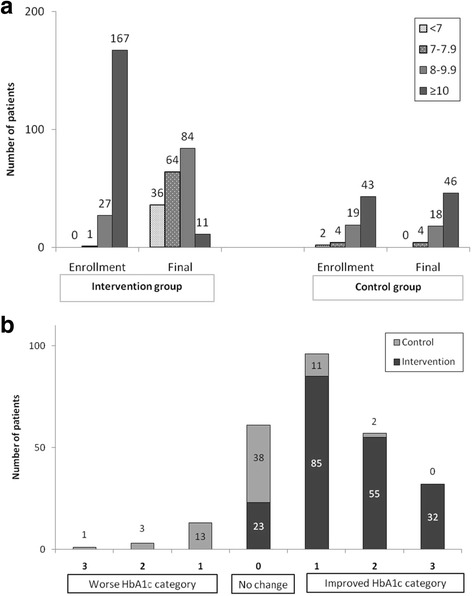
Results: In the intervention group, there were statistically significant (p < 0.05) post-intervention (relative) reductions in the levels of HbA1c (-27.1%, 95% CI = -28.9%, -25.3%), FBG (-17.10%, 95% CI = -23.3%, -10.9%), total cholesterol (-9.93%, 95% CI = -12.7%, -7.9%), LDL cholesterol (-11.4%, 95% CI = -19.4%, -3.5%), systolic BP (-1.5%, 95% CI = -2.9%, -0.03%), and diastolic BP (-3.4%, 95% CI = -5.2%, -1.7%). There was a significant decrease in the number of patients with a HbA1c ≥10 (86 mmol/mol) from 167 patients at enrollment to 11 patients after intervention (p < 0.001). However, the intervention group experienced a statistically significant increase in body weight (3.7%, 95% CI = 2.9%, 4.5%). In the control group, no statistically significant changes were noticed in different outcomes with the exception of total cholesterol (-4.10%, p = 0.07). In the linear regression model, the intervention and the total number of clinic visits predicted HbA1c improvement.
Conclusions: Implementation of a patient-specific integrated care program involving a multidisciplinary team approach, frequent clinic visits, and intensified insulin treatment was associated with marked improvement in glycemic control and cardiovascular risk factors of poorly controlled T2DM patients in a safe and reproducible manner.
Trial registration: ISRCTN Identifier: ISRCTN83437562 September 19, 2016 Retrospectively registered.
Keywords: Cardiovascular risk; Glycemic control; Multidisciplinary care; Type 2 diabetes.
Conflict of interest statement
Ethics approval and consent to participate
The Prince Sultan Military Medical City ethical committee ethically approved this study. The ethical approval number SA555 and the clinical trial is registered under the number ISRCTN83437562. This study was conducted in accordance to all Saudi regulations. The participants signed an informed consent for participation and publication.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS, Arafah MR, Khalil MZ, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25(11):1603–1610. - PubMed
-
- Al-Quwaidhi AJ, Pearce MS, Sobngwi E, Critchley JA, O’Flaherty M. Comparison of type 2 diabetes prevalence estimates in Saudi Arabia from a validated Markov model against the international diabetes federation and other modelling studies. Diabetes Res Clin Pract. 2014;103(3):496–503. doi: 10.1016/j.diabres.2013.12.036. - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention . National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2005.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
