

Predictors of In-Hospital Mortality After Rapid Response Team Calls in a 274 Hospital Nationwide Sample
- PMID: 29293147
- PMCID: PMC6044728
- DOI: 10.1097/CCM.0000000000002926
Predictors of In-Hospital Mortality After Rapid Response Team Calls in a 274 Hospital Nationwide Sample
Abstract
Objectives: Despite wide adoption of rapid response teams across the United States, predictors of in-hospital mortality for patients receiving rapid response team calls are poorly characterized. Identification of patients at high risk of death during hospitalization could improve triage to intensive care units and prompt timely reevaluations of goals of care. We sought to identify predictors of in-hospital mortality in patients who are subjects of rapid response team calls and to develop and validate a predictive model for death after rapid response team call.
Design: Analysis of data from the national Get with the Guidelines-Medical Emergency Team event registry.
Setting: Two-hundred seventy four hospitals participating in Get with the Guidelines-Medical Emergency Team from June 2005 to February 2015.
Patients: 282,710 hospitalized adults on surgical or medical wards who were subjects of a rapid response team call.
Interventions: None.
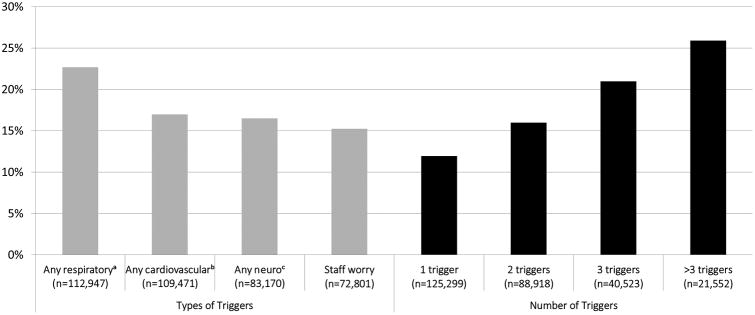
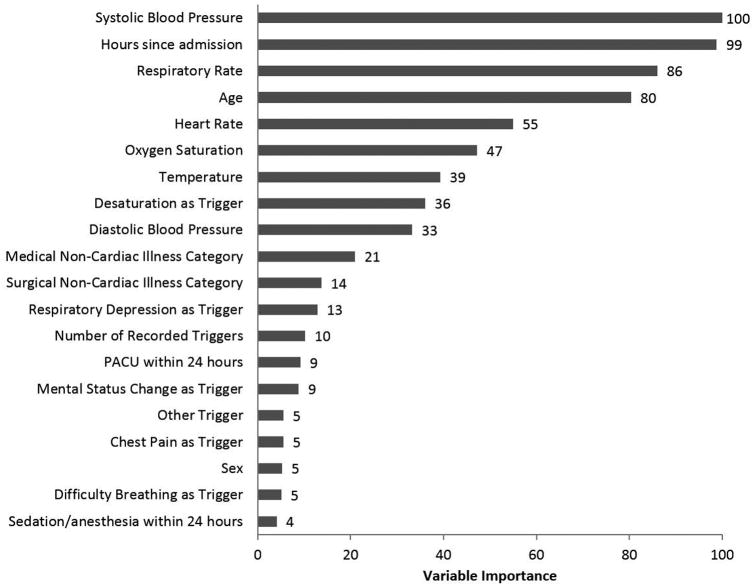
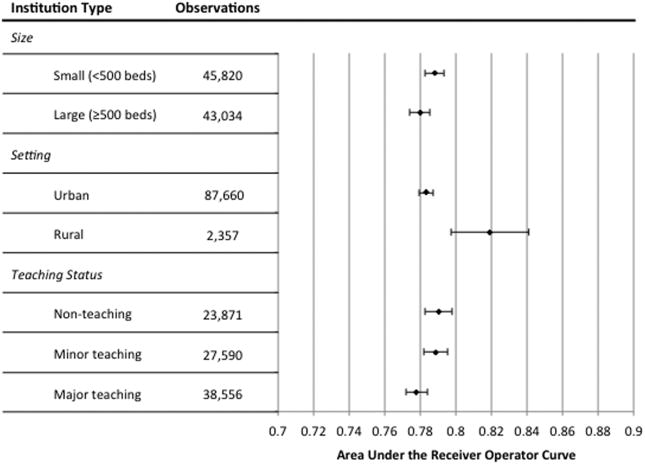
Measurements and main results: The primary outcome was death during hospitalization; candidate predictors included patient demographic- and event-level characteristics. Patients who died after rapid response team were older (median age 72 vs 66 yr), were more likely to be admitted for noncardiac medical illness (70% vs 58%), and had greater median length of stay prior to rapid response team (81 vs 47 hr) (p < 0.001 for all comparisons). The prediction model had an area under the receiver operating characteristic curve of 0.78 (95% CI, 0.78-0.79), with systolic blood pressure, time since admission, and respiratory rate being the most important variables.
Conclusions: Patients who die following rapid response team calls differ significantly from surviving peers. Recognition of these factors could improve postrapid response team triage decisions and prompt timely goals of care discussions.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
"It's Tough to Make Decisions, Especially About the Future".Crit Care Med. 2018 Jul;46(7):1181-1183. doi: 10.1097/CCM.0000000000003032. Crit Care Med. 2018. PMID: 29912096 No abstract available.
-
In-Hospital Mortality After Rapid Response Team Calls in a 274 Hospital Nationwide Sample: Does Telemetry Monitoring Have a Role to Play?Crit Care Med. 2018 Dec;46(12):e1229-e1230. doi: 10.1097/CCM.0000000000003404. Crit Care Med. 2018. PMID: 30444830 No abstract available.
-
The authors reply.Crit Care Med. 2018 Dec;46(12):e1230. doi: 10.1097/CCM.0000000000003454. Crit Care Med. 2018. PMID: 30444831 Free PMC article. No abstract available.
-
Respiratory Deterioration and Cardiac Arrest.Crit Care Med. 2019 Jan;47(1):e71-e72. doi: 10.1097/CCM.0000000000003412. Crit Care Med. 2019. PMID: 30557264 No abstract available.
References
-
- Steel AC, Reynolds SF. The growth of rapid response systems. Jt Comm J Qual Patient Saf. 2008;34(8):489–495. 433. - PubMed
-
- Priestley G, Watson W, Rashidian A, et al. Introducing Critical Care Outreach: a ward-randomised trial of phased introduction in a general hospital. Intensive Care Med. 2004;30(7):1398–1404. - PubMed
-
- Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet. 2005;365(9477):2091–2097. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
