

Risk Stratification Using Oxygenation in the First 24 Hours of Pediatric Acute Respiratory Distress Syndrome
- PMID: 29293150
- PMCID: PMC5851808
- DOI: 10.1097/CCM.0000000000002958
Risk Stratification Using Oxygenation in the First 24 Hours of Pediatric Acute Respiratory Distress Syndrome
Abstract
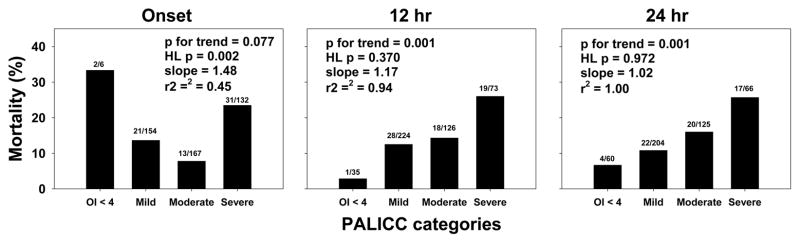
Objective: Oxygenation measured 24 hours after acute respiratory distress syndrome onset more accurately stratifies risk, relative to oxygenation at onset, in both children and adults. However, waiting 24 hours is problematic, especially for interventions that are more efficacious early in the disease course. We aimed to delineate whether oxygenation measured at timepoints earlier than 24 hours would retain predictive validity in pediatric acute respiratory distress syndrome.
Design: Observational cohort study.
Setting: Two large, academic PICUs.
Patients: Invasively ventilated children with acute respiratory distress syndrome.
Interventions: None.
Measurements and main results: PaO2/FIO2 and oxygenation index (mean airway pressure × FIO2 × 100)/PaO2) were measured at acute respiratory distress syndrome onset, at 6, 12, 18, and 24 hours after in 459 children at the Children's Hospital of Philadelphia. Neither PaO2/FIO2 nor oxygenation index at acute respiratory distress syndrome onset discriminated outcome. Between 6 and 24 hours, both PaO2/FIO2 (area under receiver operating curve for mortality between 0.57 and 0.62; p = 0.049-0.002) and oxygenation index (area under receiver operating curve, 0.60-0.62; p = 0.006-0.001) showed good discrimination and calibration across multiple outcomes, including mortality, ventilator-free days at 28 days, ventilator days in survivors, and probability of extubation, given competing risk of death. The utility of oxygenation at 12 hours was confirmed in an independent cohort from the Children's Hospital of Los Angeles.
Conclusion: Oxygenation measured between 6 and 12 hours of acute respiratory distress syndrome onset accurately stratified outcomes in children. Our results have critical implications for the design of trials, especially for interventions with greater impact in early acute respiratory distress syndrome.
Figures
Comment in
-
Estimating Pediatric Acute Respiratory Distress Syndrome Outcomes From Oxygenation Variables.Crit Care Med. 2018 Apr;46(4):654-656. doi: 10.1097/CCM.0000000000002969. Crit Care Med. 2018. PMID: 29538120 No abstract available.
References
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149(3 Pt 1):818–824. - PubMed
-
- Force ADT, Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. - PubMed
-
- Khemani RG, Thomas NJ, Venkatachalam V, et al. Comparison of SpO2 to PaO2 based markers of lung disease severity for children with acute lung injury. Crit Care Med. 2012;40(4):1309–1316. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
