

Autoimmune encephalitis epidemiology and a comparison to infectious encephalitis
- PMID: 29293273
- PMCID: PMC6011827
- DOI: 10.1002/ana.25131
Autoimmune encephalitis epidemiology and a comparison to infectious encephalitis
Abstract
Objective: To evaluate the incidence and prevalence of autoimmune encephalitis and compare it to that of infectious encephalitis.
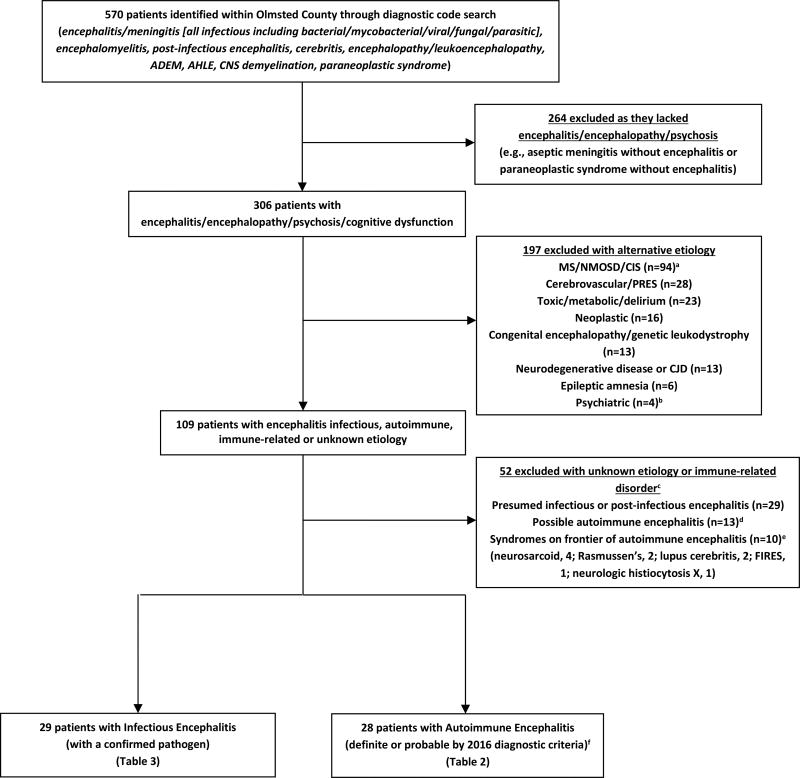
Methods: We performed a population-based comparative study of the incidence and prevalence of autoimmune and infectious encephalitis in Olmsted County, Minnesota. Autoimmune encephalitis diagnosis and subgroups were defined by 2016 diagnostic criteria, and infectious encephalitis diagnosis required a confirmed infectious pathogen. Age- and sex-adjusted prevalence and incidence rates were calculated. Patients with encephalitis of uncertain etiology were excluded.
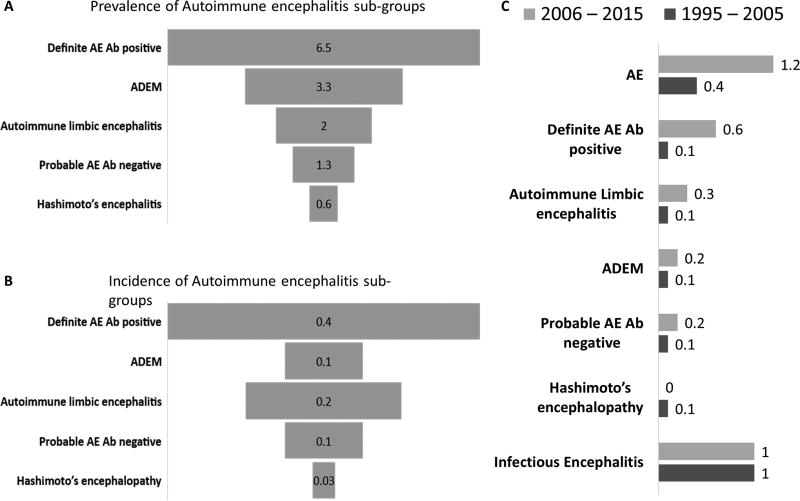
Results: The prevalence of autoimmune encephalitis on January 1, 2014 of 13.7/100,000 was not significantly different from that of all infectious encephalitides (11.6/100,000; p = 0.63) or the viral subcategory (8.3/100,000; p = 0.17). The incidence rates (1995-2015) of autoimmune and infectious encephalitis were 0.8/100,000 and 1.0/100,000 person-years, respectively (p = 0.58). The number of relapses or recurrent hospitalizations was higher for autoimmune than infectious encephalitis (p = 0.03). The incidence of autoimmune encephalitis increased over time from 0.4/100,000 person-years (1995-2005) to 1.2/100,000 person-years (2006-2015; p = 0.02), attributable to increased detection of autoantibody-positive cases. The incidence (2.8 vs 0.7/100,000 person-years, p = 0.01) and prevalence (38.3 vs 13.7/100,000, p = 0.04) of autoimmune encephalitis was higher among African Americans than Caucasians. The prevalence of specific neural autoantibodies was as follows: myelin oligodendrocyte glycoprotein, 1.9/100,000; glutamic acid decarboxylase 65, 1.9/100,000; unclassified neural autoantibody, 1.4/100,000; leucine-rich glioma-inactivated protein 1, 0.7/100,000; collapsin response-mediator protein 5, 0.7/100,000; N-methyl-D-aspartate receptor, 0.6/100,000; antineuronal nuclear antibody type 2, 0.6/100,000; and glial fibrillary acidic protein α, 0.6/100,000.
Interpretation: This study shows that the prevalence and incidence of autoimmune encephalitis are comparable to infectious encephalitis, and its detection is increasing over time. Ann Neurol 2018;83:166-177.
© 2018 American Neurological Association.
Conflict of interest statement
No authors had conflicts of interests relevant to this study.
Figures
Comment in
-
Reply to "epidemiology of autoimmune versus infectious encephalitis".Ann Neurol. 2018 May;83(5):1038. doi: 10.1002/ana.25230. Ann Neurol. 2018. PMID: 29637594 No abstract available.
-
Epidemiology of autoimmune versus infectious encephalitis.Ann Neurol. 2018 May;83(5):1037. doi: 10.1002/ana.25229. Epub 2018 Apr 30. Ann Neurol. 2018. PMID: 29637605 No abstract available.
References
-
- Vora NM, Holman RC, Mehal JM, Steiner CA, Blanton J, Sejvar J. Burden of encephalitis-associated hospitalizations in the United States, 1998–2010. Neurology. 2014;82(5):443–451. - PubMed
-
- Granerod J, Crowcroft NS. The epidemiology of acute encephalitis. Neuropsychol Rehabil. 2007;17(4–5):406–428. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
