

Baseline peripheral blood neutrophil-to-lymphocyte ratio could predict survival in patients with adult polymyositis and dermatomyositis: A retrospective observational study
- PMID: 29293605
- PMCID: PMC5749807
- DOI: 10.1371/journal.pone.0190411
Baseline peripheral blood neutrophil-to-lymphocyte ratio could predict survival in patients with adult polymyositis and dermatomyositis: A retrospective observational study
Abstract
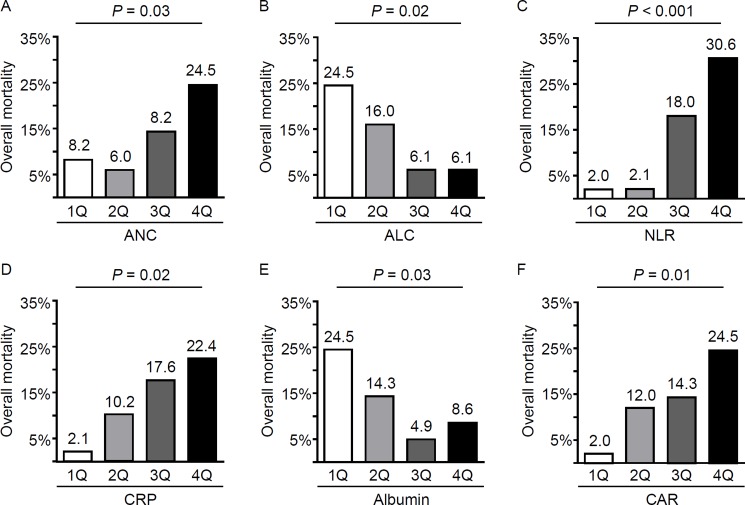
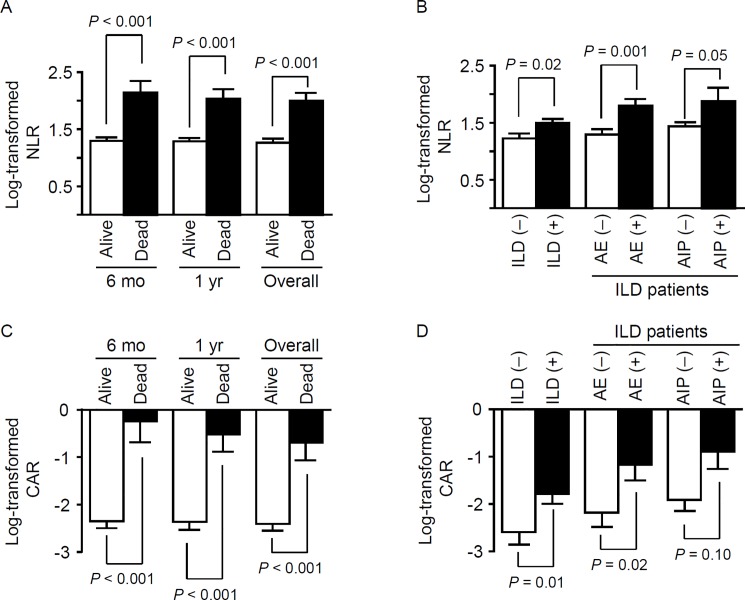
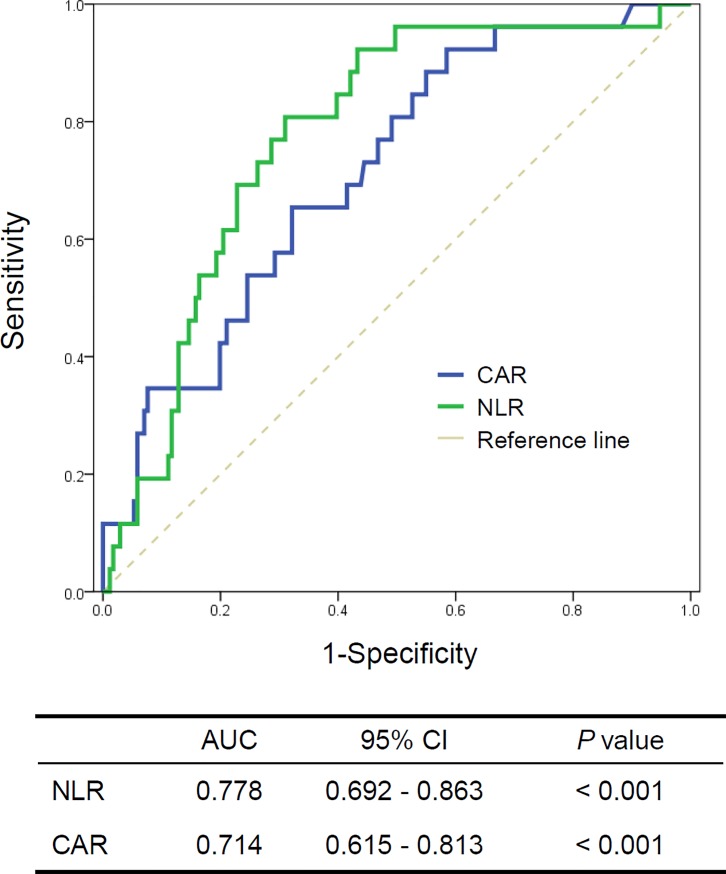
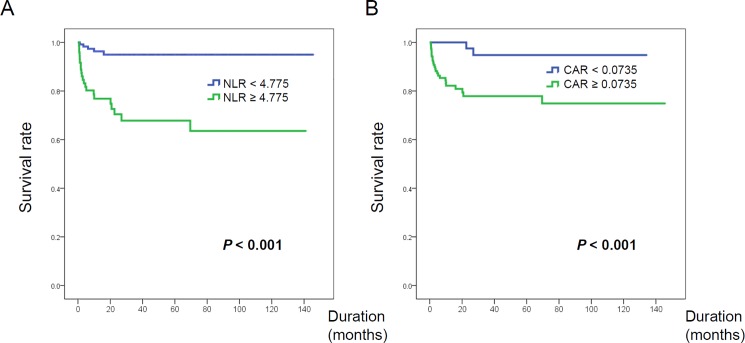
Recent studies have suggested that neutrophil-to-lymphocyte ratio (NLR) and C-reactive protein-to-albumin ratio (CAR) are emerging markers of disease activity and prognosis in patients with chronic inflammatory diseases, cardiovascular diseases, or malignancies. Therefore, we investigated the clinical significance and prognostic value of the NLR and CAR in adult patients with polymyositis and dermatomyositis. The medical records of 197 patients with newly diagnosed polymyositis/dermatomyositis between August 2003 and November 2016 were retrospectively reviewed. Survival and causes of death were recorded during an average 33-month observational period. Clinical and laboratory findings were compared between survivors and non-survivors. Using receiver operating characteristic curves, the NLR and CAR cut-off values for predicting survival were calculated. Univariate and multivariate analyses using Cox proportional hazard models were performed to identify factors associated with survival. Twenty-six patients (13.2%) died during the study period, and the 5-year survival-rate was estimated to be 82%. The non-survivor group exhibited older age and a higher prevalence of interstitial lung disease (ILD), acute interstitial pneumonia, and acute exacerbation of ILD compared to that in the survivor group. NLR and CAR values were significantly higher in the non-survivors and in patients with polymyositis/dermatomyositis-associated ILD, and the death rates increased across NLR and CAR quartiles. Furthermore, when stratified according to the NLR or CAR optimal cut-off values, patients with a high NLR (>4.775) or high CAR (>0.0735) had a significantly lower survival rate than patients with low NLR or CAR, respectively. In addition, old age (>50 years), the presence of acute interstitial pneumonia, hypoproteinemia (serum protein <5.5 g/dL), and high NLR (but not high CAR) were independent predictors for mortality. The results indicate that a high NLR is independently associated with worse overall survival. Thus, the baseline NLR level may be a simple, cost-effective prognostic marker in patients with polymyositis/dermatomyositis.
Conflict of interest statement
Figures
References
-
- Dalakas MC. Inflammatory muscle diseases. N Engl J Med. 2015;372: 1734–1747. doi: 10.1056/NEJMra1402225 - DOI - PubMed
-
- Medsger TA Jr., Robinson H, Masi AT. Factors affecting survivorship in polymyositis. A life-table study of 124 patients. Arthritis Rheum. 1971;14: 249–258. - PubMed
-
- Airio A, Kautiainen H, Hakala M. Prognosis and mortality of polymyositis and dermatomyositis patients. Clin Rheumatol. 2006;25: 234–239. doi: 10.1007/s10067-005-1164-z - DOI - PubMed
-
- Limaye V, Hakendorf P, Woodman RJ, Blumbergs P, Roberts-Thomson P. Mortality and its predominant causes in a large cohort of patients with biopsy-determined inflammatory myositis. Intern Med J. 2012;42: 191–198. doi: 10.1111/j.1445-5994.2010.02406.x - DOI - PubMed
-
- Marie I. Morbidity and mortality in adult polymyositis and dermatomyositis. Curr Rheumatol Rep. 2012;14: 275–285. doi: 10.1007/s11926-012-0249-3 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
