

Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction
- PMID: 29293969
- PMCID: PMC5939665
- DOI: 10.1093/eurheartj/ehx721
Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction
Abstract
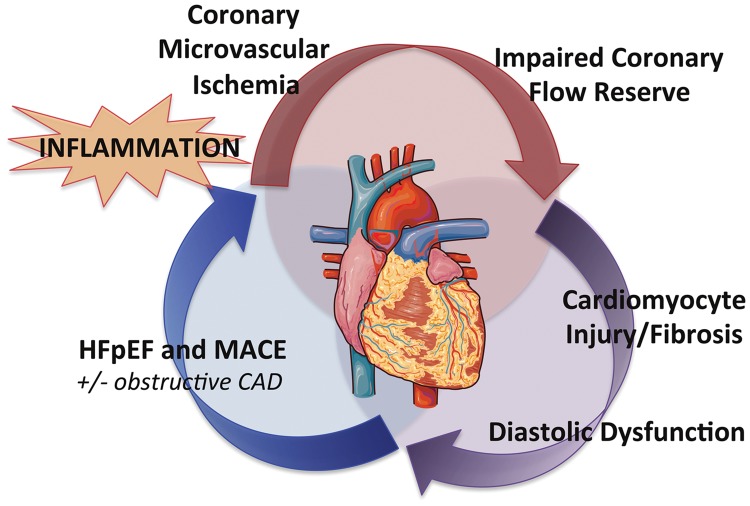
Aims: Coronary microvascular ischaemia, cardiomyocyte injury and stiffness may play an important role in the pathophysiology of heart failure with preserved ejection fraction (HFpEF). To date, the relationship between coronary flow reserve (CFR), myocardial injury, diastolic dysfunction, and future HFpEF risk is unknown.
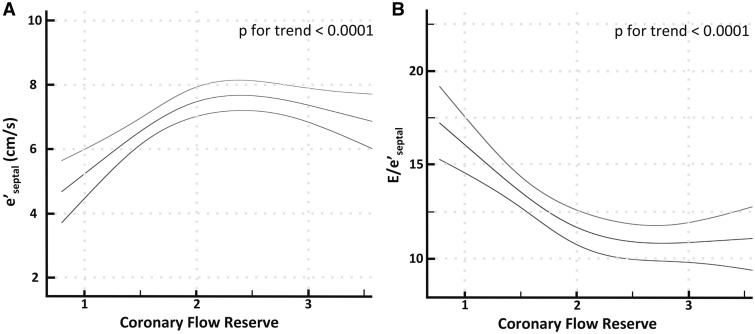
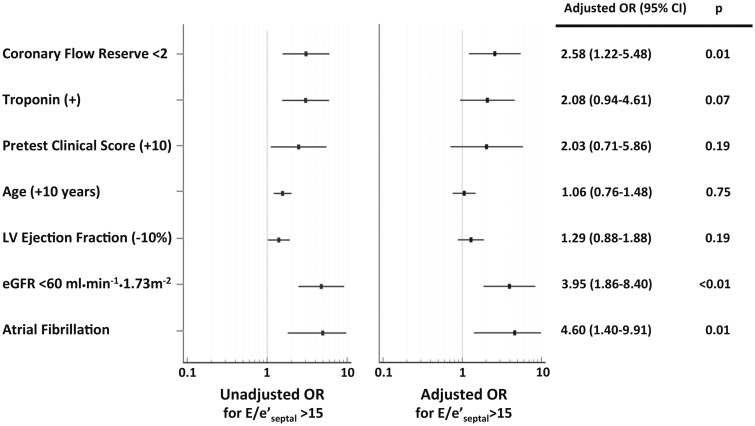
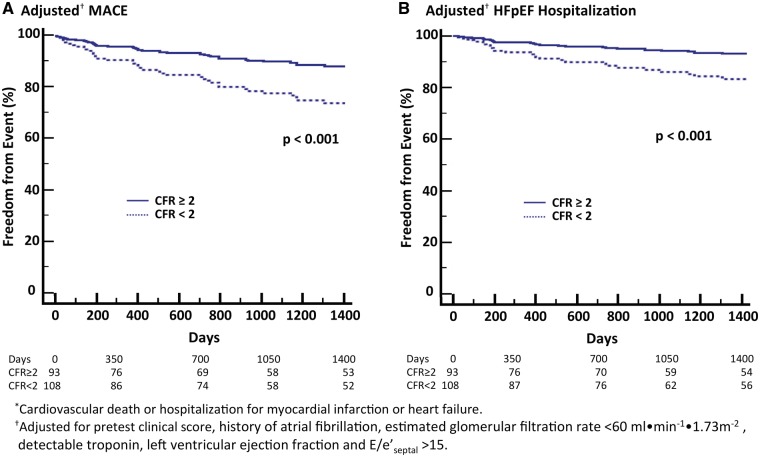
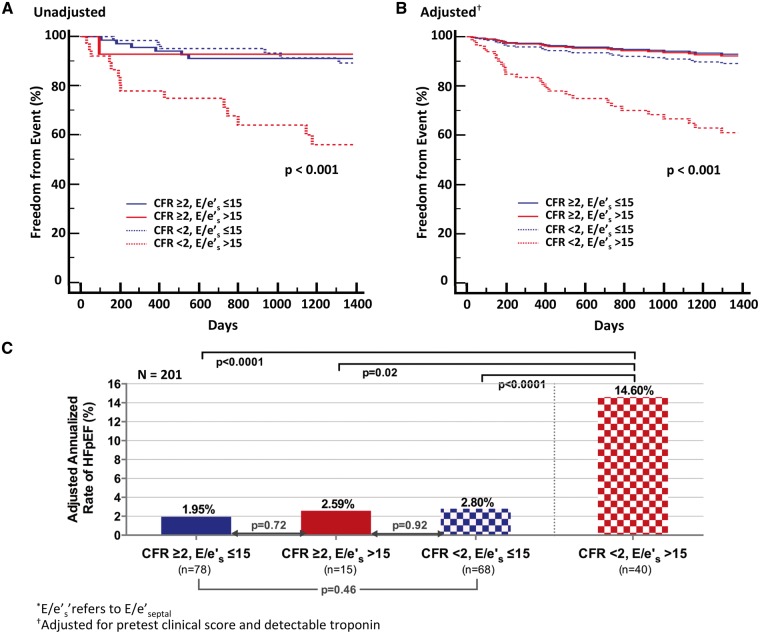
Methods and results: Consecutive patients (n = 201) undergoing evaluation for suspected coronary artery disease (CAD) with stress myocardial perfusion positron emission tomography, serum troponin, and transthoracic echocardiography who did not have flow-limiting CAD or reduced left ventricular ejection fraction were identified. Patients were followed up (median 4.1 years) for cardiovascular death and hospitalization for non-fatal myocardial infarction or heart failure. Coronary flow reserve was quantified as stress/rest myocardial blood flow. Early diastolic flow (E) and relaxation (e') velocities were obtained via transmitral and tissue Doppler, respectively. Patients with impaired CFR (<2, n = 108) demonstrated linearly decreasing e' and increasing E/e' consistent with worsening diastolic function (P for trend <0.0001). A detectable troponin was associated with diastolic dysfunction only in the presence of impaired CFR (interaction P = 0.002). In adjusted analyses, impaired CFR was independently associated with diastolic dysfunction (E/e'septal > 15, adjusted OR 2.58, 95%CI 1.22-5.48) and composite cardiovascular outcomes or HFpEF hospitalization alone (adjusted HR 2.47, 95%CI 1.09-5.62). Patients with both impaired CFR and diastolic dysfunction demonstrated >five-fold increased risk of HFpEF hospitalization (P < 0.001).
Conclusion: In symptomatic patients without overt CAD, impaired CFR was independently associated with diastolic dysfunction and adverse events, especially HFpEF hospitalization. The presence of both coronary microvascular and diastolic dysfunctions was associated with a markedly increased risk of HFpEF events.
Figures
Comment in
-
Coronary microvascular dysfunction and heart failure with preserved ejection fraction as female-pattern cardiovascular disease: the chicken or the egg?Eur Heart J. 2018 Mar 7;39(10):850-852. doi: 10.1093/eurheartj/ehx818. Eur Heart J. 2018. PMID: 29346550 Free PMC article. No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; Authors/Task Force Members. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- Redfield MM. Heart failure with preserved ejection fraction. N Engl J Med 2016;375:1868–1877. - PubMed
-
- Shah AM, Claggett B, Kitzman D, Biering-Sorensen T, Jensen JS, Cheng S, Matsushita K, Konety S, Folsom AR, Mosley TH, Wright JD, Heiss G, Solomon SD.. Contemporary assessment of left ventricular diastolic function in older adults: the atherosclerosis risk in communities study. Circulation 2017;135:426–439. - PMC - PubMed
-
- Omland T, Pfeffer MA, Solomon SD, de Lemos JA, Røsjø H, Šaltytė Benth J, Maggioni A, Domanski MJ, Rouleau JL, Sabatine MS, Braunwald E; PEACE Investigators. Prognostic value of cardiac troponin I measured with a highly sensitive assay in patients with stable coronary artery disease. J Am Coll Cardiol 2013;61:1240–1249. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
