

Frame and frameless linear accelerator-based radiosurgery for idiopathic trigeminal neuralgia
- PMID: 29296409
- PMCID: PMC5675493
Frame and frameless linear accelerator-based radiosurgery for idiopathic trigeminal neuralgia
Abstract
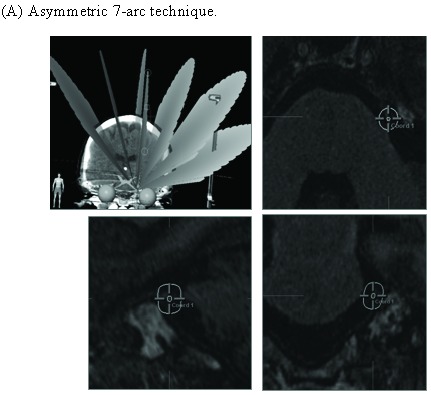
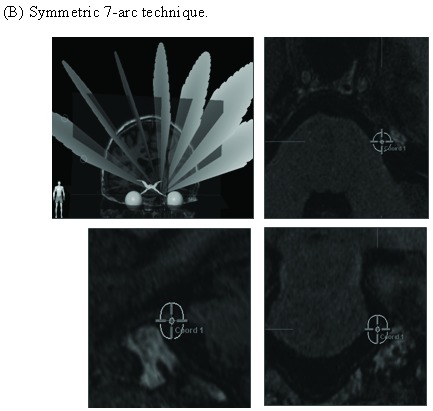
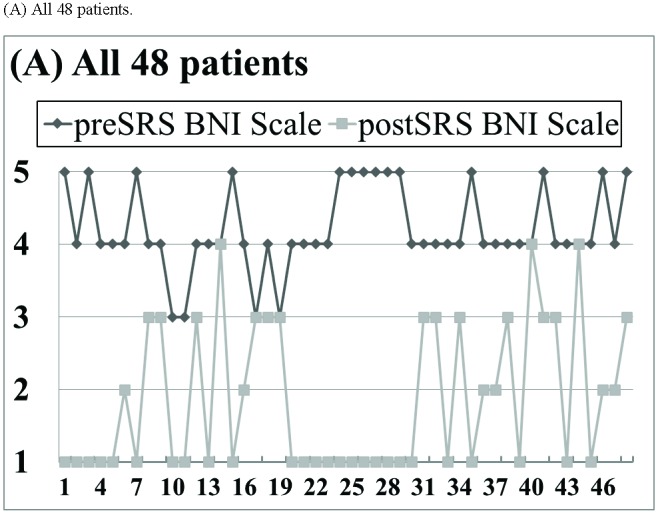
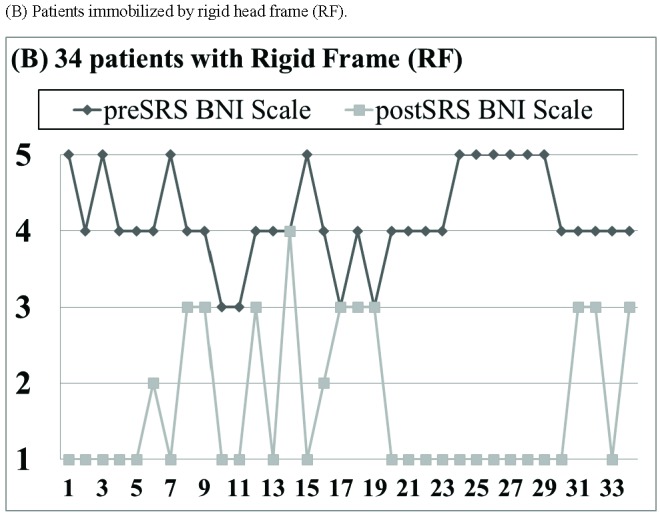
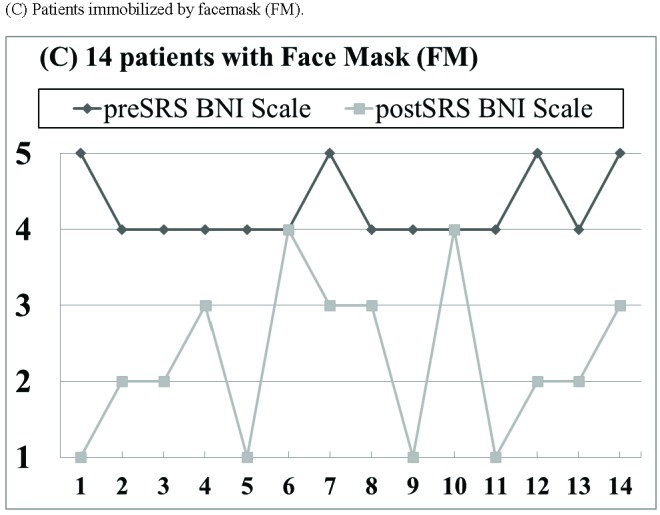
Purpose: We report outcome of linear accelerator (Linac)-based stereotactic radiosurgery (SRS) for trigeminal neuralgia (TGN) utilizing rigid head frame (RF) and facemask (FM) immobilization.Method: From November 2008 to October 2012, 48 patients with idiopathic TGN underwent primary SRS by a dedicated Linac. RF immobilization was utilized for 34 patients, and frameless image-guided radiosurgery (IGRS) with FM immobilization was performed in 14 patients. Treatment outcome was assessed by patient interviews with a 7-item questionnaire.
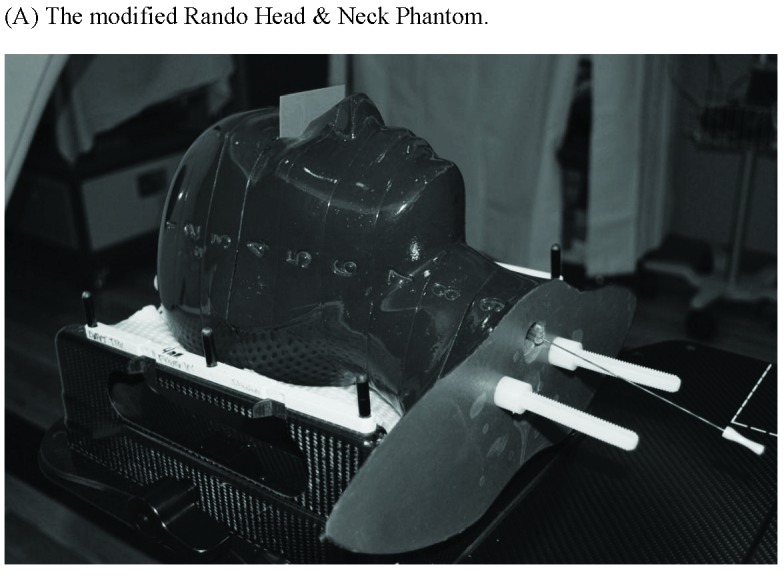
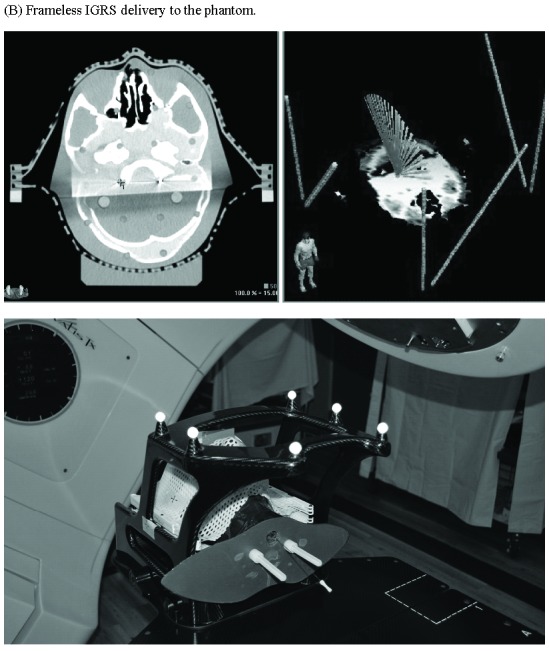
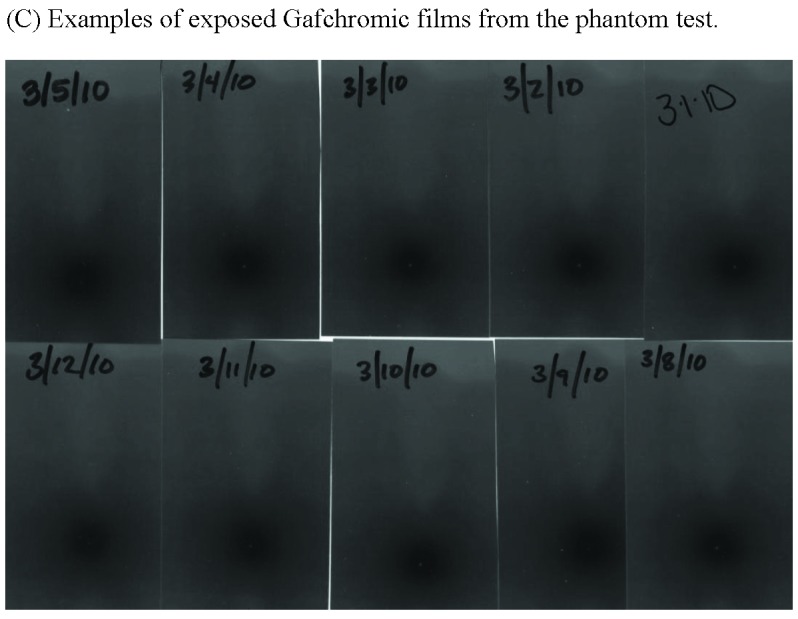
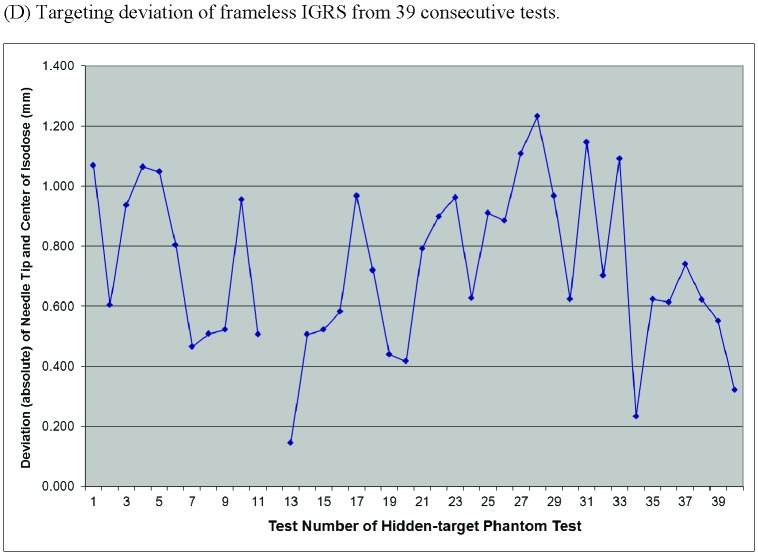
Results: Sub-millimeter targeting accuracy (0.71±0.31 mm) was recorded for frameless IGRS by a novel hidden-target phantom method. With a follow-up of 26 months, significant pain relief was recorded in 43 (89%) patients, including 26 (54%) complete and 17 (35%) partial responses; with a significant reduction of 2.4±1.3 points (p < 0.01) on the 5-point Barrow Neurological Institute pain scale. No significant pain relief difference (p = 0.23) was detected between patients immobilized by RF and FM. Notable pin site problems were reported in 9 (26%) of 34 patients immobilized by RF.
Conclusion: Frameless IGRS with FM immobilization is more patient friendly and can achieve as excellent treatment outcome as with RF immobilization for idiopathic TGN.
Keywords: frameless image-guided radiosurgery.; linear accelerator; radiosurgery; targeting accuracy; trigeminal neuralgia.
Figures
References
-
- Katusic S, Beard CM, Bergstralh E, Kurland LT. Incidence and clinical features of trigeminal neuralgia, Rochester, Minnesota, 1945–1984. Ann Neurol 1990; 27(1):89–95. - PubMed
-
- Love S, Coakham HB. Trigeminal neuralgia: pathology and pathogenesis. Brain 2001; 124:2347. - PubMed
-
- Hamlyn PJ. Neurovascular relationships in the posterior cranial fossa, with special reference to trigeminal neuralgia. 2. Neurovascular compression of the trigeminal nerve in cadaveric controls and patients with trigeminal neuralgia: quantification and influence of method. Clin Anat 1997; 10(6):380-8. - PubMed
-
- Brisman R. Trigeminal neuralgia and multiple sclerosis. Arch Neurol 1987; 44:379-381. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous