

Thrombotic thrombocytopenic purpura: diagnostic criteria, clinical features, and long-term outcomes from 1995 through 2015
- PMID: 29296701
- PMCID: PMC5728353
- DOI: 10.1182/bloodadvances.2017005124
Thrombotic thrombocytopenic purpura: diagnostic criteria, clinical features, and long-term outcomes from 1995 through 2015
Abstract
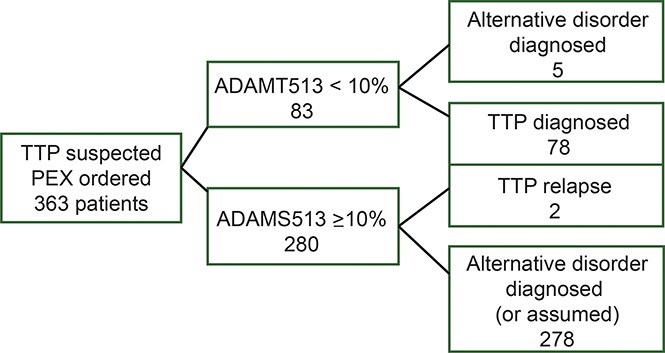
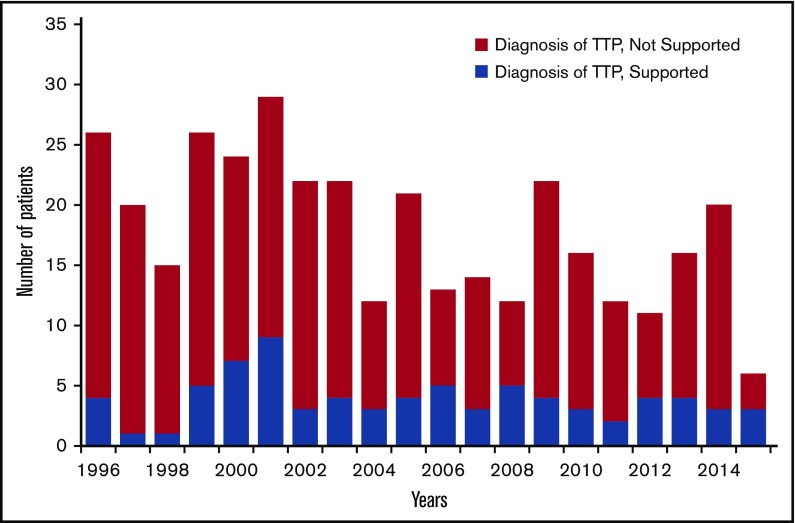
Our objective was to describe new observations from the Oklahoma Thrombotic Thrombocytopenic Purpura (TTP) Registry experience (November 1995 through December 2015) on the diagnosis of TTP along with patients' clinical features and their outcomes. Among 363 patients with an initial episode of clinically suspected TTP, the diagnosis of TTP was supported by both ADAMTS13 activity <10% and clinical features in 78 patients (21%). ADAMTS13 activity was measured in all 363 patients by 2 methods: fluorescence resonance energy transfer (FRET) and immunoblotting (IB). Sixty patients had ADAMTS13 activity <10% by both methods, 15 had ADAMTS13 <10% only by FRET, and 3 had ADAMTS13 <10% only by IB. Five patients with ADAMTS13 activity <10% by 1 method had an alternative clinical diagnosis, not TTP. Two patients with characteristic clinical features of TTP (microangiopathic hemolytic anemia and thrombocytopenia, no alternative diagnosis) and multiple relapses initially had ADAMTS13 activity >10% by both measurements. ADAMTS13 inhibitor titers were not associated with presenting features or outcomes. Microangiopathic hemolytic anemia and thrombocytopenia were not severe in all patients. Forty-seven percent of patients had no or minor neurologic abnormalities; 95% had no or minor serum creatinine abnormalities. Ten patients (13%) died, 2 before completing 1 plasma exchange (PEX); 3 deaths were attributed to PEX complications. For patients presenting after we began using rituximab in some patients (December 2003), fewer PEX treatments were required and fewer relapses occurred. Patients with their first relapse presented with higher platelet counts and hematocrits and lower lactate dehydrogenase levels and required fewer PEX treatments compared with their initial episodes.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Furlan M, Robles R, Solenthaler M, Wassmer M, Sandoz P, Lämmle B. Deficient activity of von Willebrand factor-cleaving protease in chronic relapsing thrombotic thrombocytopenic purpura. Blood. 1997;89(9):3097-3103. - PubMed
-
- Furlan M, Robles R, Galbusera M, et al. von Willebrand factor-cleaving protease in thrombotic thrombocytopenic purpura and the hemolytic-uremic syndrome. N Engl J Med. 1998;339(22):1578-1584. - PubMed
-
- Levy GG, Nichols WC, Lian EC, et al. Mutations in a member of the ADAMTS gene family cause thrombotic thrombocytopenic purpura. Nature. 2001;413(6855):488-494. - PubMed
-
- Vesely SK, George JN, Lämmle B, et al. ADAMTS13 activity in thrombotic thrombocytopenic purpura-hemolytic uremic syndrome: relation to presenting features and clinical outcomes in a prospective cohort of 142 patients. Blood. 2003;102(1):60-68. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
