

Clinicopathologic consensus study of gray zone lymphoma with features intermediate between DLBCL and classical HL
- PMID: 29296913
- PMCID: PMC5728632
- DOI: 10.1182/bloodadvances.2017009472
Clinicopathologic consensus study of gray zone lymphoma with features intermediate between DLBCL and classical HL
Abstract
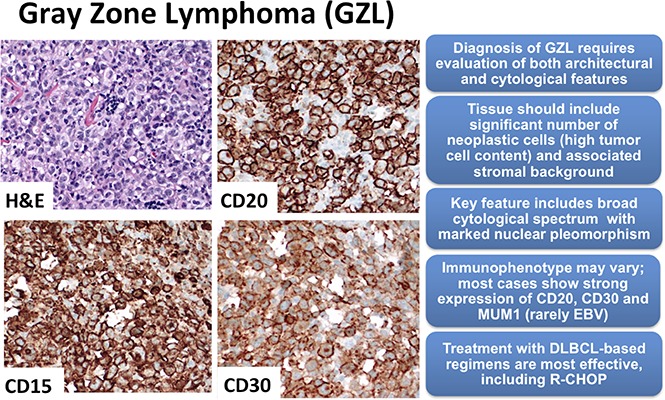
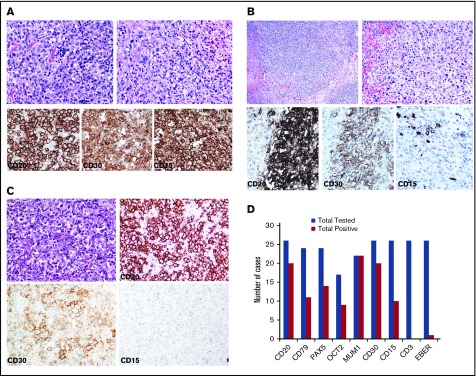
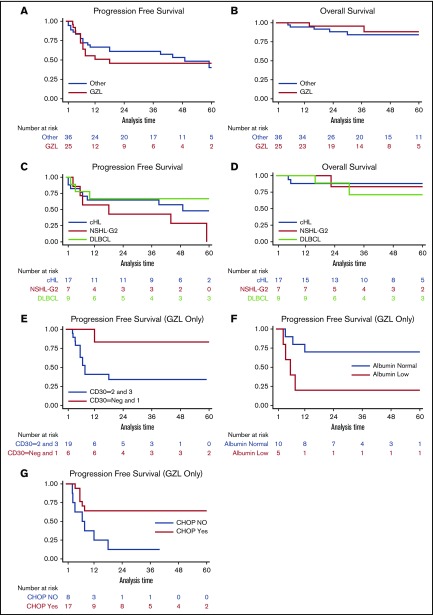
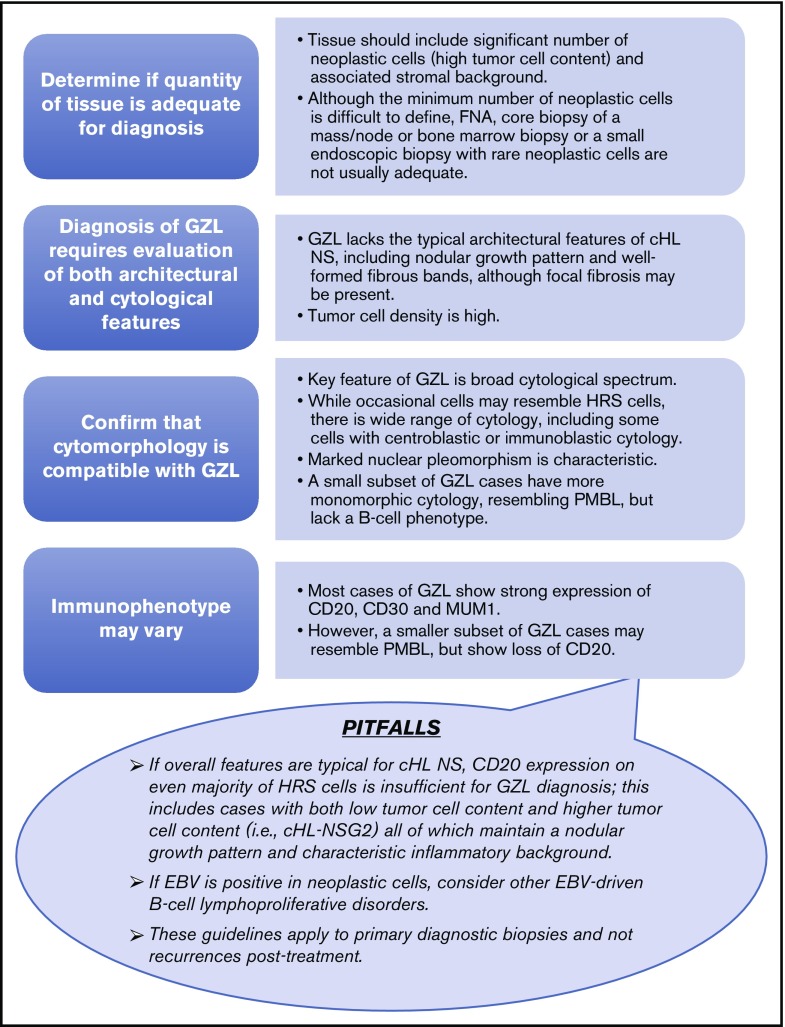
Gray zone lymphoma (GZL) is described as sharing features with classical Hodgkin lymphoma (cHL) and diffuse large B-cell lymphoma (DLBCL). However, there remains complexity in establishing diagnosis, delineating prognosis, and determining optimum therapy. Sixty-eight cases diagnosed as GZL across 15 North American academic centers were evaluated by central pathology review to achieve consensus. Of these, only 26 (38%) were confirmed as GZL. Morphology was critical to GZL consensus diagnosis (eg, tumor cell richness); immunohistochemistry showed universal B-cell derivation, frequent CD30 expression, and rare Epstein-Barr virus (EBV) positivity (CD20+, 83%; PAX5+, 100%; BCL6+, 20%; MUM1+, 100%; CD30+, 92%; EBV+, 4%). Forty-two cases were reclassified: nodular sclerosis (NS) cHL, n = 27 (including n = 10 NS grade 2); lymphocyte predominant HL, n = 4; DLBCL, n = 4; EBV+ DLBCL, n = 3; primary mediastinal large BCL n = 2; lymphocyte-rich cHL and BCL-not otherwise specified, n = 1 each. GZL consensus-confirmed vs reclassified cases, respectively, more often had mediastinal disease (69% vs 41%; P = .038) and less likely more than 1 extranodal site (0% vs 25%; P = .019). With a 44-month median follow-up, 3-year progression-free survival (PFS) and overall survival for patients with confirmed GZL were 39% and 95%, respectively, vs 58% and 85%, respectively, for reclassified cases (P = .19 and P = .15, respectively). Interestingly, NS grade 2 reclassified patients had similar PFS as GZL consensus-confirmed cases. For prognostication of GZL cases, hypoalbuminemia was a negative factor (3-year PFS, 12% vs 64%; P = .01), whereas frontline cyclophosphamide, doxorubicin, vincristine, and prednisone ± rituximab (CHOP±R) was associated with improved 3-year PFS (70% vs 20%; P = .03); both factors remained significant on multivariate analysis. Altogether, accurate diagnosis of GZL remains challenging, and improved therapeutic strategies are needed.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Traverse-Glehen A, Pittaluga S, Gaulard P, et al. Mediastinal gray zone lymphoma: the missing link between classic Hodgkin’s lymphoma and mediastinal large B-cell lymphoma. Am J Surg Pathol. 2005;29(11):1411-1421. - PubMed
-
- García JF, Mollejo M, Fraga M, et al. Large B-cell lymphoma with Hodgkin’s features. Histopathology. 2005;47(1):101-110. - PubMed
-
- Evens AM, Kanakry JA, Sehn LH, et al. Gray zone lymphoma with features intermediate between classical Hodgkin lymphoma and diffuse large B-cell lymphoma: characteristics, outcomes, and prognostication among a large multicenter cohort. Am J Hematol. 2015;90(9):778-783. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
