

Network meta-analysis of randomized trials in multiple myeloma: efficacy and safety in relapsed/refractory patients
- PMID: 29296961
- PMCID: PMC5738982
- DOI: 10.1182/bloodadvances.2016003905
Network meta-analysis of randomized trials in multiple myeloma: efficacy and safety in relapsed/refractory patients
Abstract
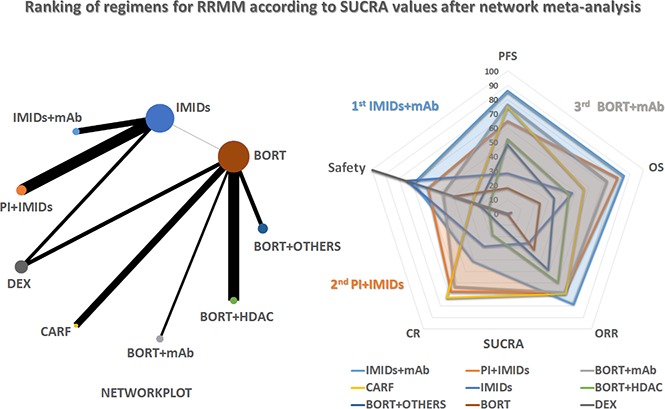
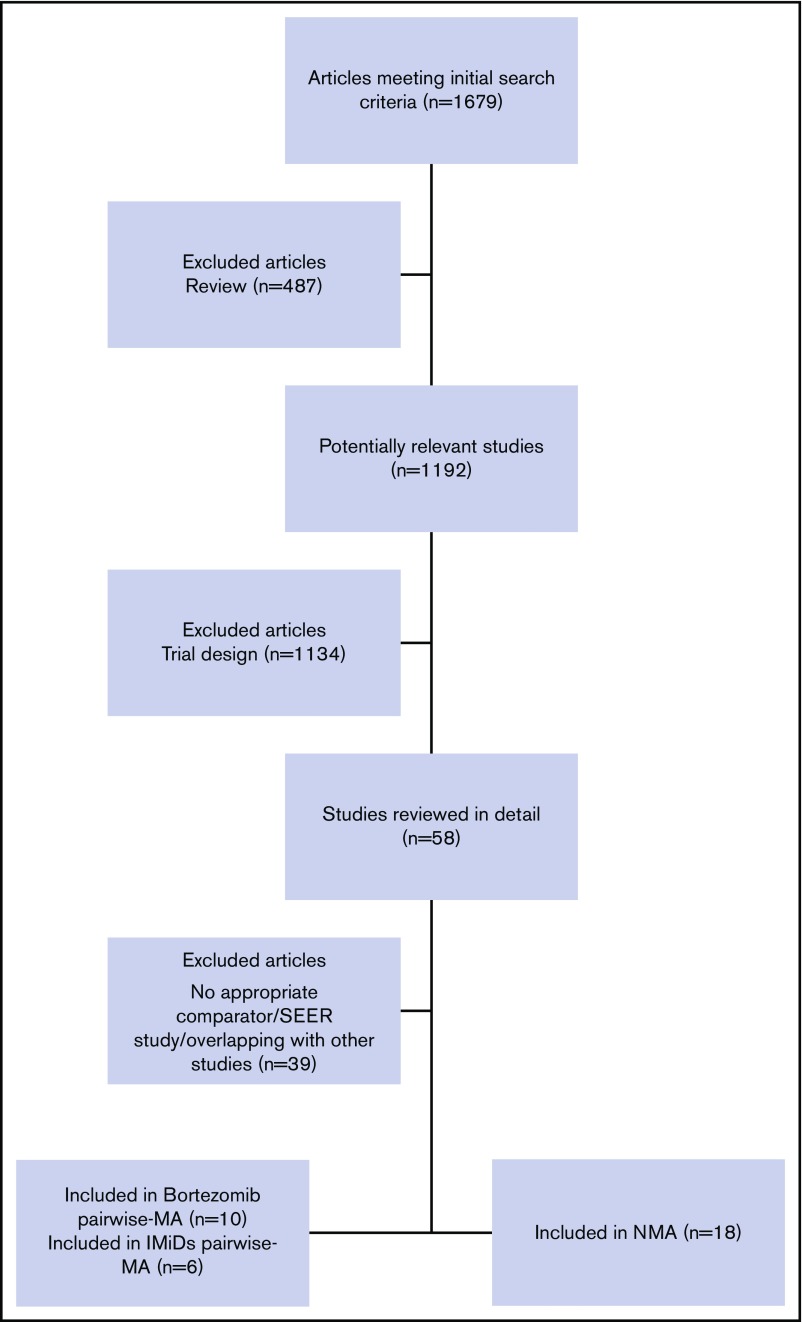
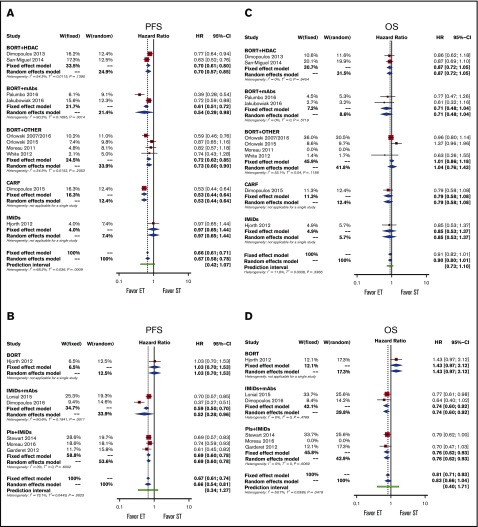
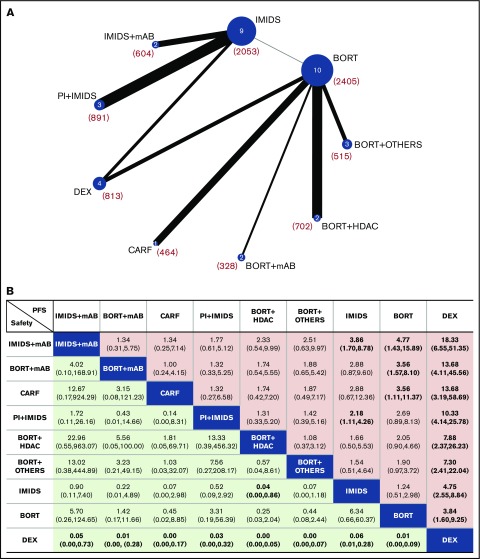
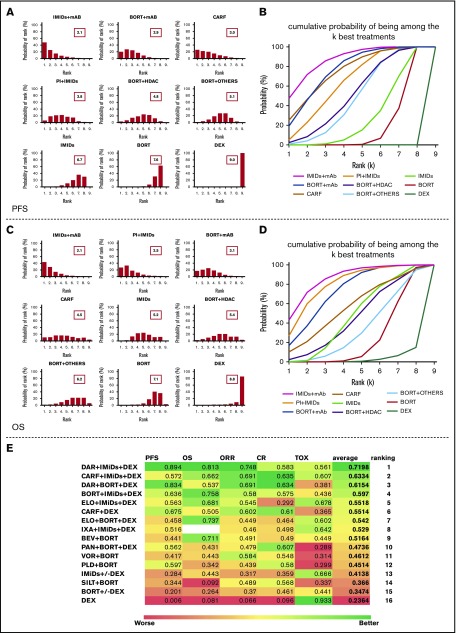
Despite major therapeutic advancements, multiple myeloma (MM) is still incurable and relapsed/refractory multiple myeloma (RRMM) remains a challenge; the rational choice of the most appropriate regimen in this setting is currently undefined. We performed a systematic review and 2 standard pairwise meta-analyses to evaluate the efficacy of regimens that have been directly compared with bortezomib or immunomodulatory imide drugs (IMiDs) in head-to-head clinical trials and a network meta-analysis (NMA) to determine the relevance of each regimen on the basis of all the available direct and indirect evidence. Sixteen trials were included in the pairwise meta-analyses, and 18 trials were included in the NMA. Pairwise meta-analyses showed that a 3-drug regimen (bortezomib- or IMiD-based) was superior to a 2-drug regimen in progression-free-survival (PFS) and overall response rate (ORR). NMA showed that an IMiD backbone associated with anti-MM monoclonal antibodies (mAbs) (preferably) or proteasome inhibitors had the highest probability of being the most effective regimen with the lowest toxicity. The combination of daratumumab, lenalidomide, and dexamethasone ranked as the first regimen in terms of activity, efficacy, and tolerability according to the average value between surface under the cumulative ranking curve of PFS, overall survival, ORR, complete response rate, and safety. This is the first NMA comparing all currently available regimens evaluated in published randomized trials for the treatment of RRMM, but our results need to be interpreted taking into account differences in their patient populations. Our analysis suggests that IMiDs plus new anti-MM mAb-containing regimens are the most active therapeutic option in RRMM.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Laubach J, Garderet L, Mahindra A, et al. Management of relapsed multiple myeloma: recommendations of the International Myeloma Working Group. Leukemia. 2016;30(5):1005-1017. - PubMed
-
- Ludwig H, Miguel JS, Dimopoulos MA, et al. International Myeloma Working Group recommendations for global myeloma care. Leukemia. 2014;28(5):981-992. - PubMed
-
- Moreau P, Attal M, Facon T. Frontline therapy of multiple myeloma. Blood. 2015;125(20):3076-3084. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
