

Differences in Morbidity and Mortality Rates in Black, White, and Hispanic Very Preterm Infants Among New York City Hospitals
- PMID: 29297054
- PMCID: PMC5796743
- DOI: 10.1001/jamapediatrics.2017.4402
Differences in Morbidity and Mortality Rates in Black, White, and Hispanic Very Preterm Infants Among New York City Hospitals
Abstract
Importance: Substantial quality improvements in neonatal care have occurred over the past decade yet racial and ethnic disparities in morbidity and mortality remain. It is uncertain whether disparate patterns of care by race and ethnicity contribute to disparities in neonatal outcomes.
Objectives: To examine differences in neonatal morbidity and mortality rates among non-Hispanic black (black), Hispanic, and non-Hispanic white (white) very preterm infants and to determine whether these differences are explained by site of delivery.
Design, setting, and participants: Population-based retrospective cohort study of 7177 nonanomalous infants born between 24 and 31 completed gestational weeks in 39 New York City hospitals using linked 2010 to 2014 New York City discharge abstract and birth certificate data sets. Mixed-effects logistic regression with a random hospital-specific intercept was used to generate risk-adjusted neonatal morbidity and mortality rates for very preterm infants in each hospital. Hospitals were ranked using this measure, and differences in the distribution of black, Hispanic, and white very preterm births were assessed among these hospitals. The statistical analysis was performed in 2016-2017.
Exposure: Race/ethnicity.
Main outcomes and measures: Composite of mortality (neonatal or in-hospital up to 1 year) or severe neonatal morbidity (bronchopulmonary dysplasia, severe necrotizing enterocolitis, retinopathy of prematurity stage 3 or greater, or intraventricular hemorrhage grade 3 or greater).
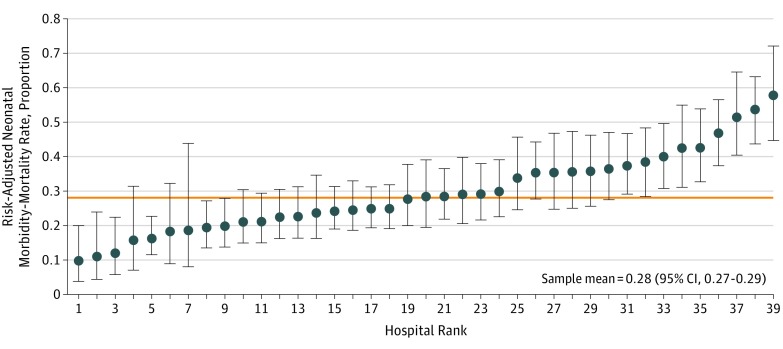
Results: Among 7177 very preterm births (VPTBs), morbidity and mortality occurred in 2011 (28%) and was higher among black (893 [32.2%]) and Hispanic (610 [28.1%]) than white (319 [22.5%]) VPTBs (2-tailed P < .001). The risk-standardized morbidity and mortality rate was twice as great for VPTB infants born in hospitals in the highest morbidity and mortality tertile (0.40; 95% CI, 0.38-0.41) as for those born in the lowest morbidity and mortality tertile (0.16; 95% CI, 0.14-0.18). Black (1204 of 2775 [43.4%]) and Hispanic (746 of 2168 [34.4%]) VPTB infants were more likely than white (325 of 1418 [22.9%]) VPTB infants to be born in hospitals in the highest morbidity and mortality tertile (2-tailed P < .001; black-white difference, 20%; 95% CI, 18%-23% and Hispanic-white difference, 11%; 95% CI, 9%-14%). The largest proportion of the explained disparities can be attributed to differences in infant health risks among black, Hispanic, and white VPTB infants. However, 40% (95% CI, 30%-50%) of the black-white disparity and 30% (95% CI, 10%-49%) of the Hispanic-white disparity was explained by birth hospital.
Conclusions and relevance: Black and Hispanic VPTB infants are more likely to be born at hospitals with higher risk-adjusted neonatal morbidity and mortality rates, and these differences contribute to excess morbidity and mortality among black and Hispanic infants.
Conflict of interest statement
Figures
Comment in
-
Choice of Hospital as a Source of Racial/Ethnic Disparities in Neonatal Mortality and Morbidity Rates.JAMA Pediatr. 2018 Mar 1;172(3):221-223. doi: 10.1001/jamapediatrics.2017.4917. JAMA Pediatr. 2018. PMID: 29297051 No abstract available.
References
-
- Horbar JD, Edwards EM, Greenberg LT, et al. . Variation in performance of neonatal intensive care units in the United States. JAMA Pediatr. 2017;171(3):e164396. - PubMed
-
- Lorch SA. A decade of improvement in neonatal intensive care: how do we continue the momentum? JAMA Pediatr. 2017;171(3):e164395. - PubMed
-
- Horbar JD, Carpenter JH, Badger GJ, et al. . Mortality and neonatal morbidity among infants 501 to 1500 grams from 2000 to 2009. Pediatrics. 2012;129(6):1019-1026. - PubMed
-
- Lapcharoensap W, Gage SC, Kan P, et al. . Hospital variation and risk factors for bronchopulmonary dysplasia in a population-based cohort. JAMA Pediatr. 2015;169(2):e143676. - PubMed
-
- Matthews TJ, MacDorman MF, Thoma ME. Infant mortality statistics from the 2013 period linked birth/infant death data set. Natl Vital Stat Rep. 2015;64(9):1-30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
