

The bloody mess of red blood cell transfusion
- PMID: 29297368
- PMCID: PMC5751535
- DOI: 10.1186/s13054-017-1912-x
The bloody mess of red blood cell transfusion
Abstract
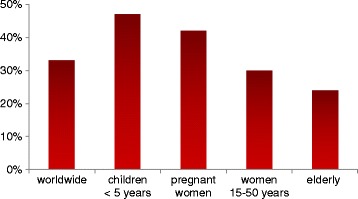
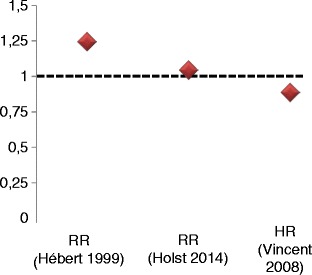
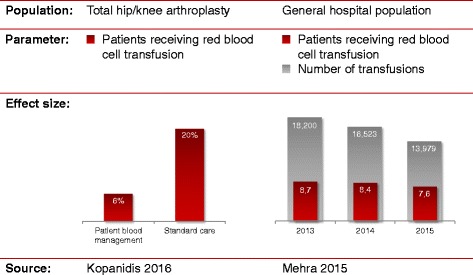
Red blood cell (RBC) transfusion might be life-saving in settings with acute blood loss, especially uncontrolled haemorrhagic shock. However, there appears to be a catch-22 situation reflected by the facts that preoperative anaemia represents an independent risk factor for postoperative morbidity and mortality, and that RBC transfusion might also contribute to adverse clinical outcomes. This dilemma is further complicated by the difficulty to define the "best" transfusion trigger and strategy. Since one size does obviously not fit all, a personalised approach is merited. Attempts should thus be made to critically reflect on the pros and cons of RBC transfusion in each individual patient. Patient blood management concepts including preoperative, intraoperative and postoperative optimisation strategies involving the intensive care unit are warranted and are likely to provide benefits for the patients and the healthcare system. In this context, it is important to consider that "simply" increasing the haemoglobin content, and in proportion oxygen delivery, may not necessarily contribute to a better outcome but potentially the contrary in the long term. The difficulty lies in identification of the patients who might eventually profit from RBC transfusion and to determine in whom a transfusion might be withheld without inducing harm. More robust clinical data providing long-term outcome data are needed to better understand in which patients RBC transfusion might be life-saving vs life-limiting.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
MW is the Chief Medical Officer of Fresenius Kabi AG. HK is Senior Vice President Global Medical, Clinical & Regulatory Affairs of Fresenius Kabi. The authors state that they have no competing interests concerning the submitted article.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Docherty AB, O’Donnell R, Brunskill S, Trivella M, Doree C, Holst L, Parker M, Gregersen M, Pinheiro de Almeida J, Walsh TS, Stanworth SJ. Effect of restrictive versus liberal transfusion strategies on outcomes in patients with cardiovascular disease in a non-cardiac surgery setting: systematic review and meta-analysis. BMJ. 2016;352:i1351. doi: 10.1136/bmj.i1351. - DOI - PMC - PubMed
-
- Nakamura RE, Vincent J, Fukushima JT, de Almeida JP, Franco RA, Lee Park C, Osawa EA, Pinto Silva CM, Costa Auler JO, Landoni G, Barbosa Gomes Galas FR, Filho RK, Hajjar LA. A liberal strategy of red blood cell transfusion reduces cardiogenic shock in elderly patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2015;150:1314–1320. doi: 10.1016/j.jtcvs.2015.07.051. - DOI - PubMed
-
- World Health Organization (WHO). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. http://www.who.int/vmnis/indicators/haemoglobin.pdf.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
