

Personalized physiological medicine
- PMID: 29297391
- PMCID: PMC5751773
- DOI: 10.1186/s13054-017-1907-7
Personalized physiological medicine
Abstract
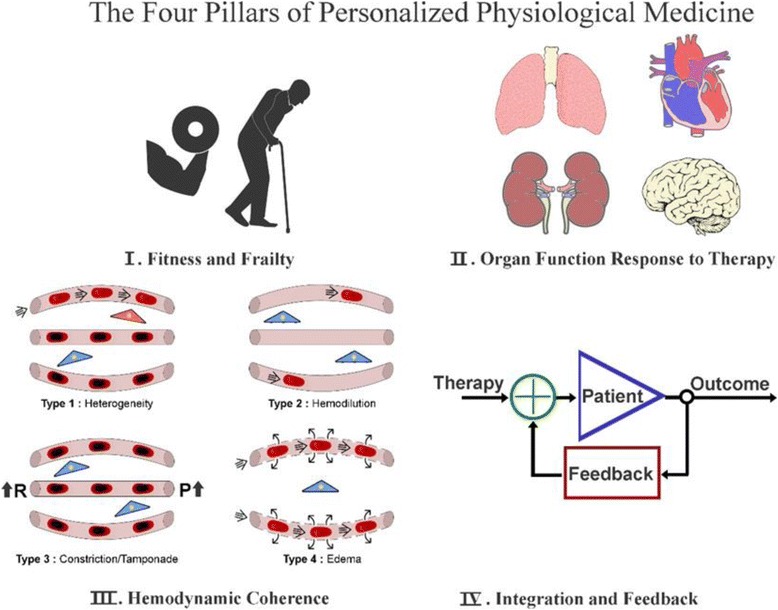
This paper introduces the concept of personalized physiological medicine that is specifically directed at the needs of the critically ill patient. This differs from the conventional view of personalized medicine, characterized by biomarkers and gene profiling, instead focusing on time-variant changes in the pathophysiology and regulation of various organ systems and their cellular and subcellular constituents. I propose that personalized physiological medicine is composed of four pillars relevant to the critically ill patient. Pillar 1 is defined by the frailty and fitness of the patient and their physiological reserve to cope with the stress of critical illness and therapy. Pillar 2 involves monitoring of the key physiological variables of the different organ systems and their response to disease and therapy. Pillar 3 concerns the evaluation of the success of resuscitation by assessment of the hemodynamic coherence between the systemic and microcirculation and parenchyma of the organ systems. Finally, pillar 4 is defined by the integration of the physiological and clinical data into a time-learning adaptive model of the patient to provide feedback about the function of organ systems and to guide and assess the response to disease and therapy. I discuss each pillar and describe the challenges to research and development that will allow the realization of personalized physiological medicine to be practiced at the bedside for critically ill patients.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable to this paper.
Consent for publication
Not applicable to this paper.
Competing interests
CI has received honoraria and independent research grants from Fresenius-Kabi (Bad Homburg, Germany), Baxter Health Care (Deerfield, Illinois), and AM-Pharma (Bunnik, The Netherlands). He has developed SDF imaging and is listed as the inventor on related patents commercialized by MicroVision Medical (MVM) under a license from the Academic Medical Center (AMC). He has been a consultant for MVM in the past, but has not been involved with this company for more than 5 years and holds no shares in this company. Braedius Medical, a company owned by a relative of CI, has developed and designed a hand-held microscope called CytoCam-IDF imaging. CI has no financial relation with Braedius Medical of any sort, i.e., never owned shares, or received consultancy or speaker fees from Braedius Medical. CI hosts an internet site (
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Calvano SE, Xiao W, Richards DR, Felciano RM, Baker HV, Cho RJ, Chen RO, Brownstein BH, Cobb JP, Tschoeke SK, Miller-Graziano C, Moldawer LL, Mindrinos MN, Davis RW, Tompkins RG, Lowry SF. A network-based analysis of systemic inflammation in humans. Nature. 2005;437(7061):1032–7. doi: 10.1038/nature03985. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
