

The Vienna psychosocial assessment procedure for bionic reconstruction in patients with global brachial plexus injuries
- PMID: 29298304
- PMCID: PMC5751989
- DOI: 10.1371/journal.pone.0189592
The Vienna psychosocial assessment procedure for bionic reconstruction in patients with global brachial plexus injuries
Abstract
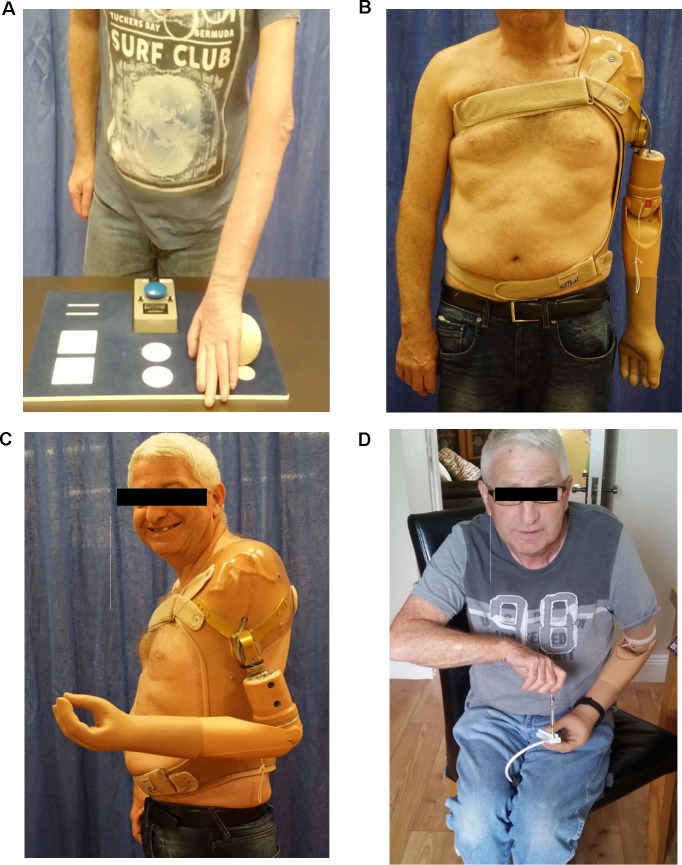
Background: Global brachial plexopathies cause major sensory and motor deficits in the affected arm and hand. Many patients report of psychosocial consequences including chronic pain, decreased self-sufficiency, and poor body image. Bionic reconstruction, which includes the amputation and prosthetic replacement of the functionless limb, has been shown to restore hand function in patients where classic reconstructions have failed. Patient selection and psychological evaluation before such a life-changing procedure are crucial for optimal functional outcomes. In this paper we describe a psychosocial assessment procedure for bionic reconstruction in patients with complete brachial plexopathies and present psychosocial outcome variables associated with bionic reconstruction.
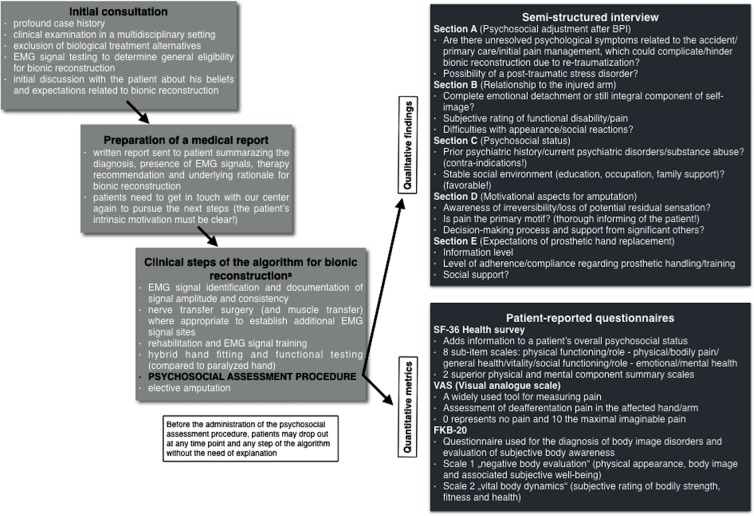
Methods: Between 2013 and 2017 psychosocial assessments were performed in eight patients with global brachial plexopathies. We conducted semi-structured interviews exploring the psychosocial adjustment related to the accident, the overall psychosocial status, as well as motivational aspects related to an anticipated amputation and expectations of functional prosthetic outcome. During the interview patients were asked to respond freely. Their answers were transcribed verbatim by the interviewer and analyzed afterwards on the basis of a pre-defined item scoring system. The interview was augmented by quantitative evaluation of self-reported mental health and social functioning (SF-36 Health Survey), body image (FKB-20) and deafferentation pain (VAS). Additionally, psychosocial outcome variables were presented for seven patients before and after bionic reconstruction.
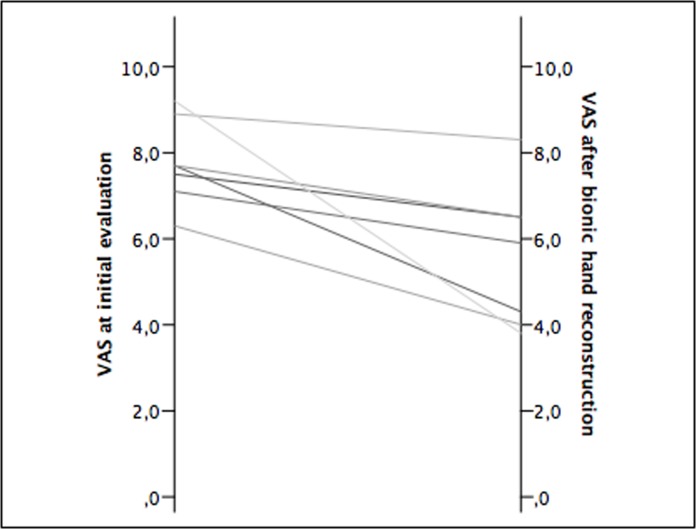
Results: Qualitative data revealed several psychological stressors with long-term negative effects on patients with complete brachial plexopathies. 88% of patients felt functionally limited to a great extent due to their disability, and all of them reported constant, debilitating pain in the deafferented hand. After bionic reconstruction the physical component summary scale increased from 30.80 ± 5.31 to 37.37 ± 8.41 (p-value = 0.028), the mental component summary scale improved from 43.19 ± 8.32 to 54.76 ± 6.78 (p-value = 0.018). VAS scores indicative of deafferentation pain improved from 7.8 to 5.6 after prosthetic hand replacement (p-value = 0.018). Negative body evaluation improved from 60.71 ± 12.12 to 53.29 ± 11.03 (p-value = 0.075). Vital body dynamics increased from 38.57 ± 13.44 to 44.43 ± 16.15 (p-value = 0.109).
Conclusions: Bionic reconstruction provides hope for patients with complete brachial plexopathies who have lived without hand function for years or even decades. Critical patient selection is crucial and the psychosocial assessment procedure including a semi-structured interview helps identify unresolved psychological issues, which could preclude or delay bionic reconstruction. Bionic reconstruction improves overall quality of life, restores an intact self-image and reduces deafferentation pain.
Conflict of interest statement
Figures
References
-
- Beisteiner R, Hollinger I, Rath J, Wurnig M, Hilbert M, Klinger N, et al. New type of cortical neuroplasticity after nerve repair in brachial plexus lesions. Archives of neurology. 2011;68(11):1467–70. doi: 10.1001/archneurol.2011.596 . - DOI - PubMed
-
- Bertelli JA, Ghizoni MF. Reconstruction of complete palsies of the adult brachial plexus by root grafting using long grafts and nerve transfers to target nerves. J Hand Surg Am. 2010;35(10):1640–6. doi: 10.1016/j.jhsa.2010.06.019 . - DOI - PubMed
-
- Terzis JK, Papakonstantinou KC. The surgical treatment of brachial plexus injuries in adults. Plast Reconstr Surg. 2000;106(5):1097–122; quiz 123–4. . - PubMed
-
- Alnot JY. Traumatic brachial plexus lesions in the adult. Indications and results. Hand Clin. 1995;11(4):623–31. . - PubMed
-
- Kim DH, Cho YJ, Tiel RL, Kline DG. Outcomes of surgery in 1019 brachial plexus lesions treated at Louisiana State University Health Sciences Center. Journal of neurosurgery. 2003;98(5):1005–16. doi: 10.3171/jns.2003.98.5.1005 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
