

Cultural adaptation of a peer-led lifestyle intervention program for diabetes prevention in India: the Kerala diabetes prevention program (K-DPP)
- PMID: 29298703
- PMCID: PMC6389141
- DOI: 10.1186/s12889-017-4986-0
Cultural adaptation of a peer-led lifestyle intervention program for diabetes prevention in India: the Kerala diabetes prevention program (K-DPP)
Abstract
Background: Type 2 diabetes mellitus (T2DM) is now one of the leading causes of disease-related deaths globally. India has the world's second largest number of individuals living with diabetes. Lifestyle change has been proven to be an effective means by which to reduce risk of T2DM and a number of "real world" diabetes prevention trials have been undertaken in high income countries. However, systematic efforts to adapt such interventions for T2DM prevention in low- and middle-income countries have been very limited to date. This research-to-action gap is now widely recognised as a major challenge to the prevention and control of diabetes. Reducing the gap is associated with reductions in morbidity and mortality and reduced health care costs. The aim of this article is to describe the adaptation, development and refinement of diabetes prevention programs from the USA, Finland and Australia to the State of Kerala, India.
Methods: The Kerala Diabetes Prevention Program (K-DPP) was adapted to Kerala, India from evidence-based lifestyle interventions implemented in high income countries, namely, Finland, United States and Australia. The adaptation process was undertaken in five phases: 1) needs assessment; 2) formulation of program objectives; 3) program adaptation and development; 4) piloting of the program and its delivery; and 5) program refinement and active implementation.
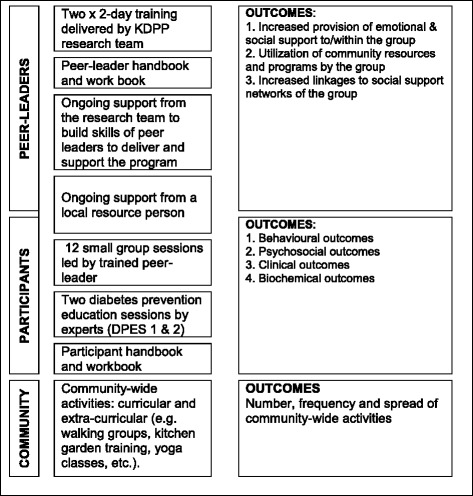
Results: The resulting program, K-DPP, includes four key components: 1) a group-based peer support program for participants; 2) a peer-leader training and support program for lay people to lead the groups; 3) resource materials; and 4) strategies to stimulate broader community engagement. The systematic approach to adaptation was underpinned by evidence-based behavior change techniques.
Conclusion: K-DPP is the first well evaluated community-based, peer-led diabetes prevention program in India. Future refinement and utilization of this approach will promote translation of K-DPP to other contexts and population groups within India as well as other low- and middle-income countries. This same approach could also be applied more broadly to enable the translation of effective non-communicable disease prevention programs developed in high-income settings to create context-specific evidence in rapidly developing low- and middle-income countries.
Trial registration: Australia and New Zealand Clinical Trials Registry: ACTRN12611000262909 . Registered 10 March 2011.
Keywords: Community-based; Cultural adaptation; Diabetes prevention; Implementation; Lifestyle intervention; Low and middle income countries (LMICs); Peer support; Type 2 diabetes mellitus (T2DM).
Conflict of interest statement
Ethics approval and consent to participate
The research was approved by the Institutional Ethics Committee of the Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, India (SCT/IEC-333/May 2011), and by the Human Research Ethics Committee of Monash University, Australia (CF11/0457-2,011,000,194) and the University of Melbourne, Australia (1441736). The trial was registered on the Australia and New Zealand Clinical Trials Registry: ACTRN12611000262909.
All study participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
A peer-support lifestyle intervention for preventing type 2 diabetes in India: A cluster-randomized controlled trial of the Kerala Diabetes Prevention Program.PLoS Med. 2018 Jun 6;15(6):e1002575. doi: 10.1371/journal.pmed.1002575. eCollection 2018 Jun. PLoS Med. 2018. PMID: 29874236 Free PMC article. Clinical Trial.
-
A group-based lifestyle intervention for diabetes prevention in low- and middle-income country: implementation evaluation of the Kerala Diabetes Prevention Program.Implement Sci. 2018 Jul 18;13(1):97. doi: 10.1186/s13012-018-0791-0. Implement Sci. 2018. PMID: 30021592 Free PMC article. Clinical Trial.
-
Cost-effectiveness of a lifestyle intervention in high-risk individuals for diabetes in a low- and middle-income setting: Trial-based analysis of the Kerala Diabetes Prevention Program.BMC Med. 2020 Sep 4;18(1):251. doi: 10.1186/s12916-020-01704-9. BMC Med. 2020. PMID: 32883279 Free PMC article. Clinical Trial.
-
The effect of community-based programs on diabetes prevention in low- and middle-income countries: a systematic review and meta-analysis.Global Health. 2019 Feb 1;15(1):10. doi: 10.1186/s12992-019-0451-4. Global Health. 2019. PMID: 30709362 Free PMC article.
-
[Steps toward the primary prevention of type II diabetes mellitus. Various epidemiological considerations].Invest Clin. 1997 Mar;38(1):39-52. Invest Clin. 1997. PMID: 9235072 Review. Spanish.
Cited by
-
The Development of Text Messages to Support People at Risk of Diabetes in Low-Resourced Communities: The South African Diabetes Prevention Programme.Nutrients. 2023 Nov 5;15(21):4692. doi: 10.3390/nu15214692. Nutrients. 2023. PMID: 37960345 Free PMC article.
-
A peer-support lifestyle intervention for preventing type 2 diabetes in India: A cluster-randomized controlled trial of the Kerala Diabetes Prevention Program.PLoS Med. 2018 Jun 6;15(6):e1002575. doi: 10.1371/journal.pmed.1002575. eCollection 2018 Jun. PLoS Med. 2018. PMID: 29874236 Free PMC article. Clinical Trial.
-
Enhanced or hindered research benefits? A realist review of community engagement and participatory research practices for non-communicable disease prevention in low- and middle-income countries.BMJ Glob Health. 2024 Feb 10;9(2):e013712. doi: 10.1136/bmjgh-2023-013712. BMJ Glob Health. 2024. PMID: 38341191 Free PMC article. Review.
-
The effect of a cluster-randomized controlled trial on lifestyle behaviors among families at risk for developing type 2 diabetes across Europe: the Feel4Diabetes-study.Int J Behav Nutr Phys Act. 2021 Jul 1;18(1):86. doi: 10.1186/s12966-021-01153-4. Int J Behav Nutr Phys Act. 2021. PMID: 34210333 Free PMC article. Clinical Trial.
-
The relationship between common mental disorders and incident diabetes among participants in the Kerala Diabetes Prevention Program (K-DPP).PLoS One. 2021 Jul 23;16(7):e0255217. doi: 10.1371/journal.pone.0255217. eCollection 2021. PLoS One. 2021. PMID: 34297780 Free PMC article. Clinical Trial.
References
-
- International Diabetes Federation . Diabetes Atlas - 7th Edition. Brussels, Belgium: International Diabetes Federation; 2015.
-
- Ramachandran A, Snehalatha C, Mary S, Selvam S, Kumar CK, Seeli AC, Shetty AS. Pioglitazone does not enhance the effectiveness of lifestyle modification in preventing conversion of impaired glucose tolerance to diabetes in Asian Indians: results of the Indian diabetes prevention Programme-2 (IDPP-2). Diabetologia. 2009:1019–26. - PubMed
-
- Thankappan KR, Shah B, Mathur P, Sarma PS, Srinivas G, Mini GK, Soman MDB, Vasan RS. Risk factor profile for chronic non-communicable diseases: results of a community-based study in Kerala, India. Indian J Med Res. 2010;131:53–63. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
