

Intravenous delivery of oncolytic reovirus to brain tumor patients immunologically primes for subsequent checkpoint blockade
- PMID: 29298869
- PMCID: PMC6276984
- DOI: 10.1126/scitranslmed.aam7577
Intravenous delivery of oncolytic reovirus to brain tumor patients immunologically primes for subsequent checkpoint blockade
Abstract
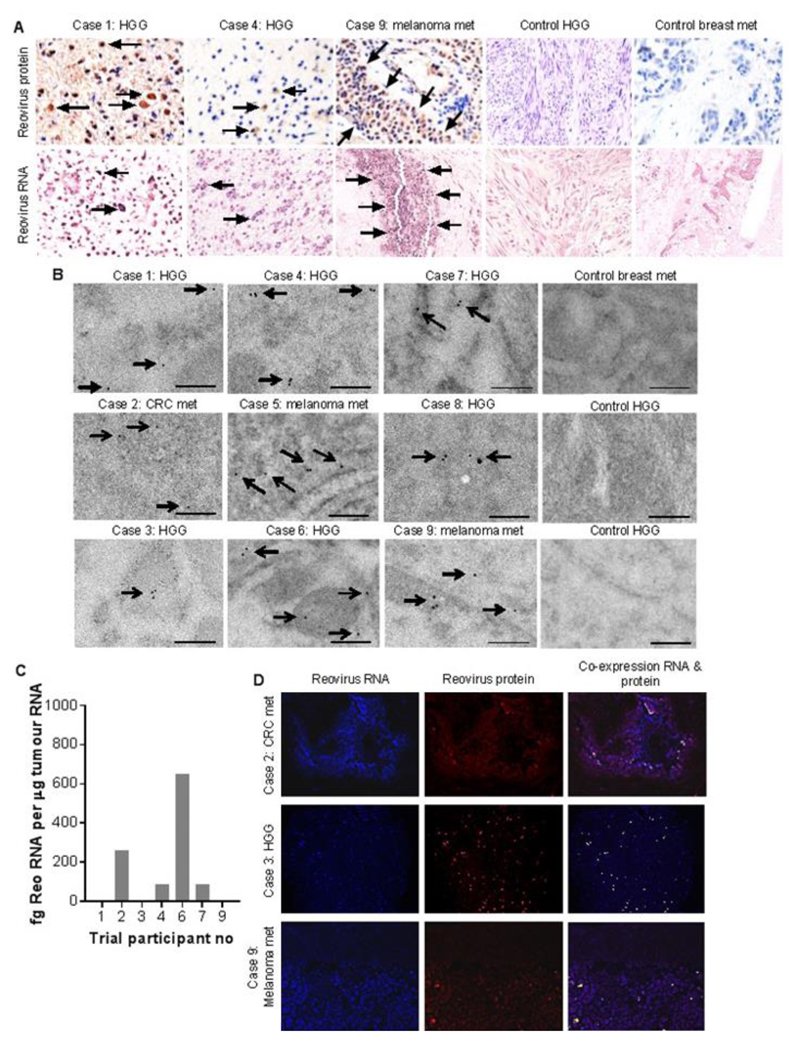
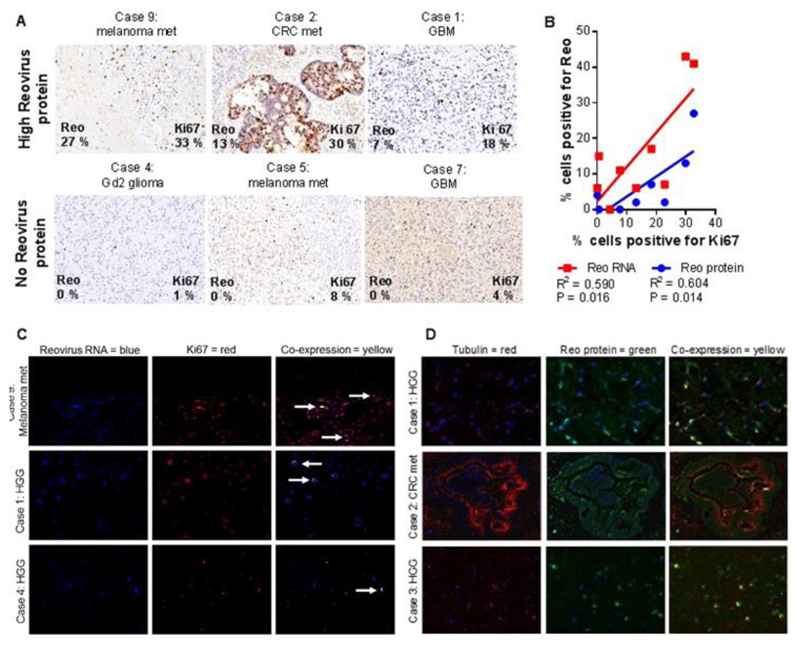
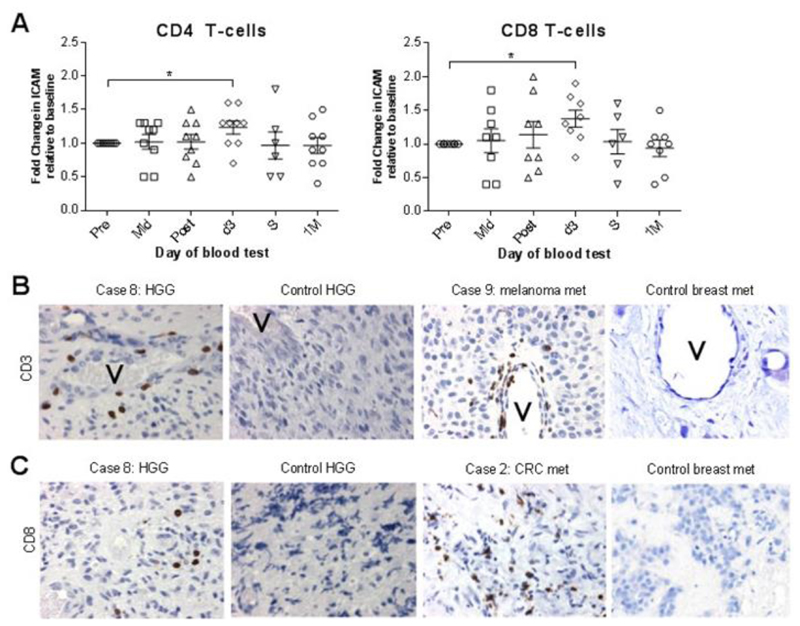
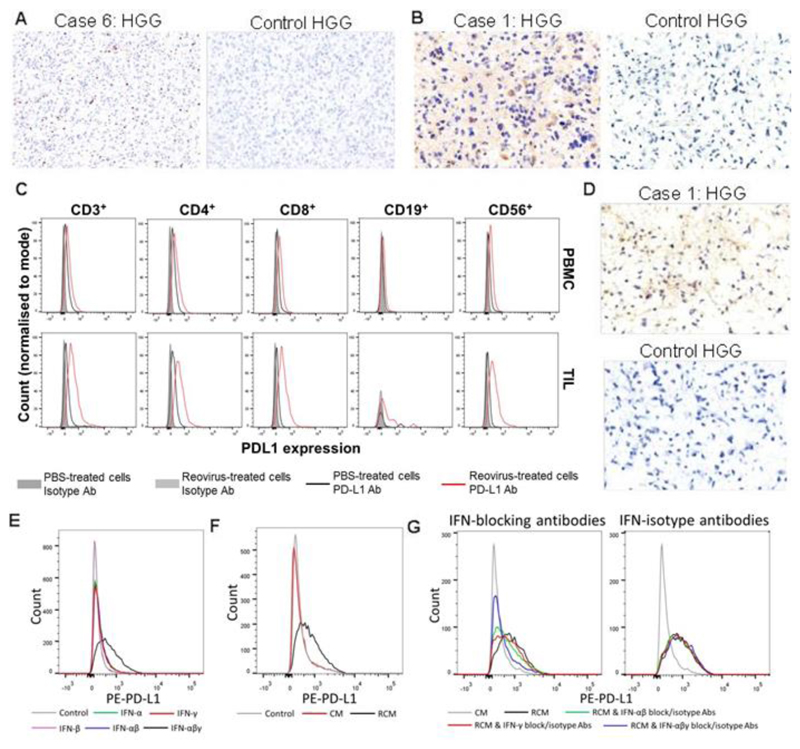
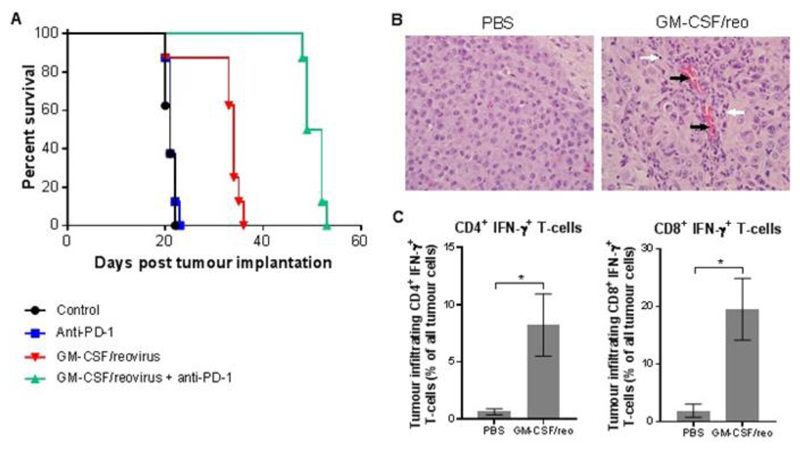
Immune checkpoint inhibitors, including those targeting programmed cell death protein 1 (PD-1), are reshaping cancer therapeutic strategies. Evidence suggests, however, that tumor response and patient survival are determined by tumor programmed death ligand 1 (PD-L1) expression. We hypothesized that preconditioning of the tumor immune microenvironment using targeted, virus-mediated interferon (IFN) stimulation would up-regulate tumor PD-L1 protein expression and increase cytotoxic T cell infiltration, improving the efficacy of subsequent checkpoint blockade. Oncolytic viruses (OVs) represent a promising form of cancer immunotherapy. For brain tumors, almost all studies to date have used direct intralesional injection of OV, because of the largely untested belief that intravenous administration will not deliver virus to this site. We show, in a window-of-opportunity clinical study, that intravenous infusion of oncolytic human Orthoreovirus (referred to herein as reovirus) leads to infection of tumor cells subsequently resected as part of standard clinical care, both in high-grade glioma and in brain metastases, and increases cytotoxic T cell tumor infiltration relative to patients not treated with virus. We further show that reovirus up-regulates IFN-regulated gene expression, as well as the PD-1/PD-L1 axis in tumors, via an IFN-mediated mechanism. Finally, we show that addition of PD-1 blockade to reovirus enhances systemic therapy in a preclinical glioma model. These results support the development of combined systemic immunovirotherapy strategies for the treatment of both primary and secondary tumors in the brain.
Copyright © 2018 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures
Comment in
-
Immunotherapy: Viral reprogramming.Nat Rev Cancer. 2018 Mar;18(3):135. doi: 10.1038/nrc.2018.12. Epub 2018 Feb 9. Nat Rev Cancer. 2018. PMID: 29422599 No abstract available.
References
-
- Robert C, Long GV, Brady B, Dutriaux C, Maio M, Mortier L, Hassel JC, Rutkowski P, McNeil C, Kalinka-Warzocha E, Savage KJ, et al. Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N Engl J Med. 2014 141116004513004. - PubMed
-
- Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, Tykodi SS, Sosman JA, Procopio G, Plimack ER, Castellano D, et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med. 2015 150925150201006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
