

A pictorial review of reconstructive foot and ankle surgery: evaluation and intervention of the flatfoot deformity
- PMID: 29299095
- PMCID: PMC5743145
- DOI: 10.3941/jrcr.v11i6.2757
A pictorial review of reconstructive foot and ankle surgery: evaluation and intervention of the flatfoot deformity
Abstract
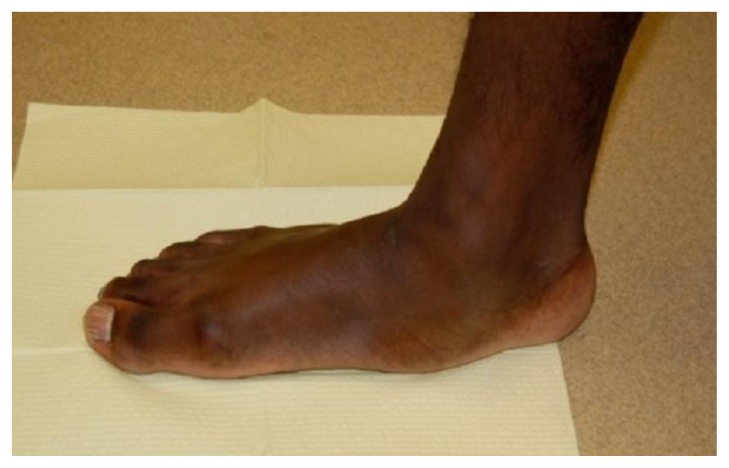
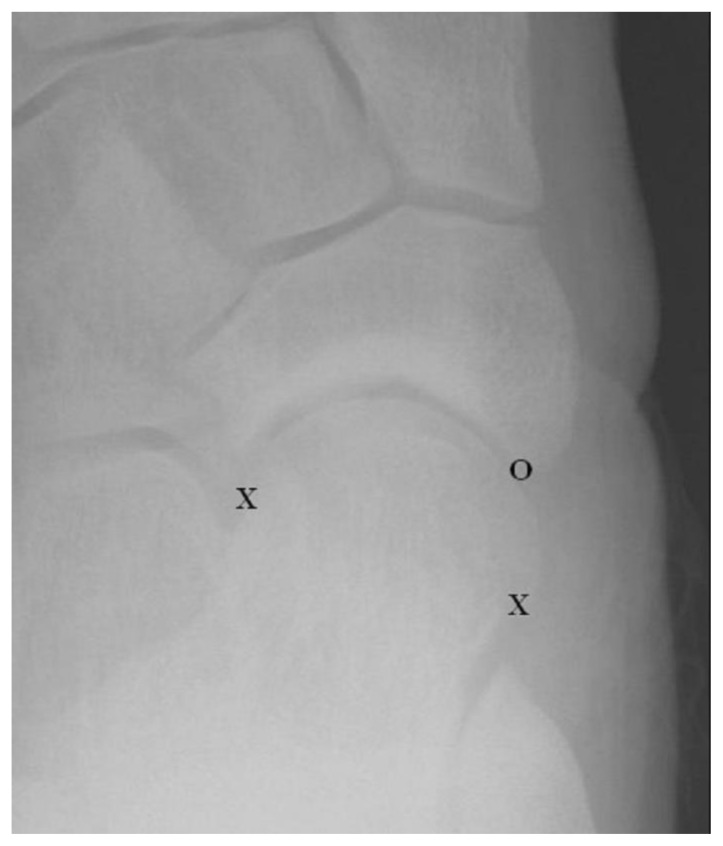
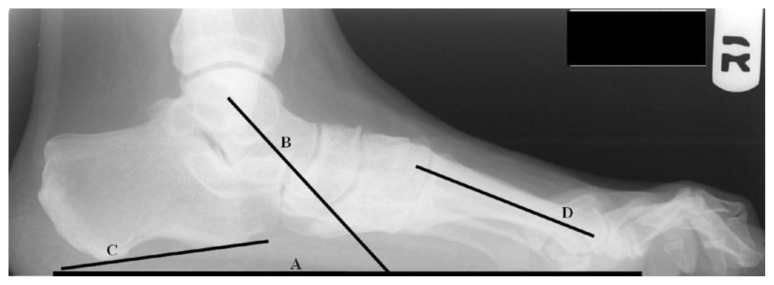
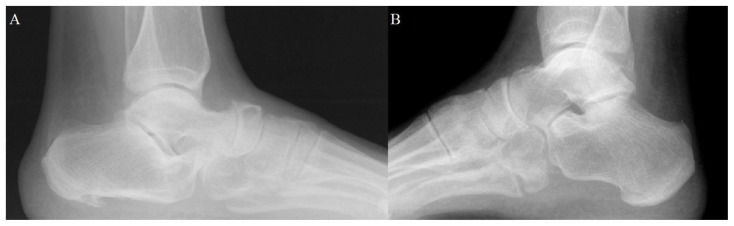
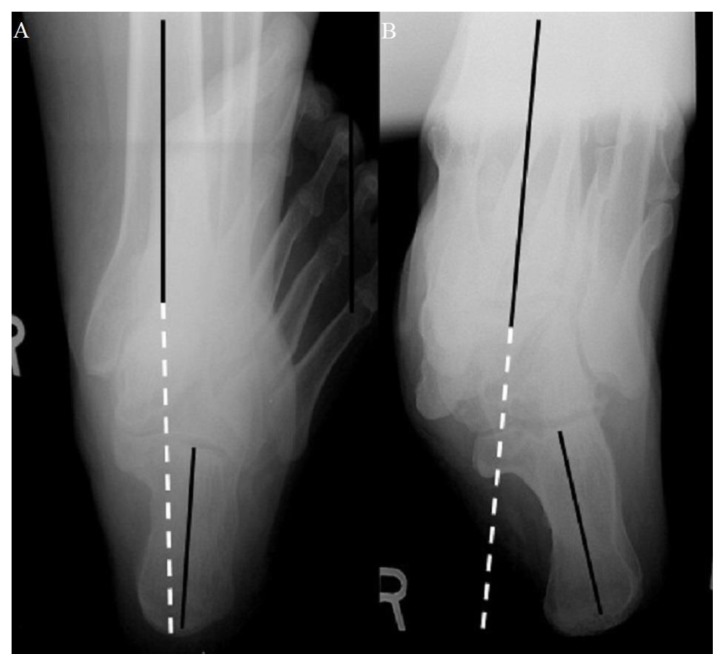
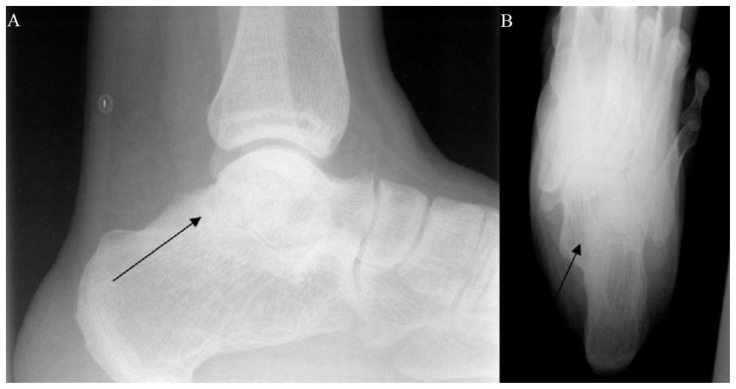
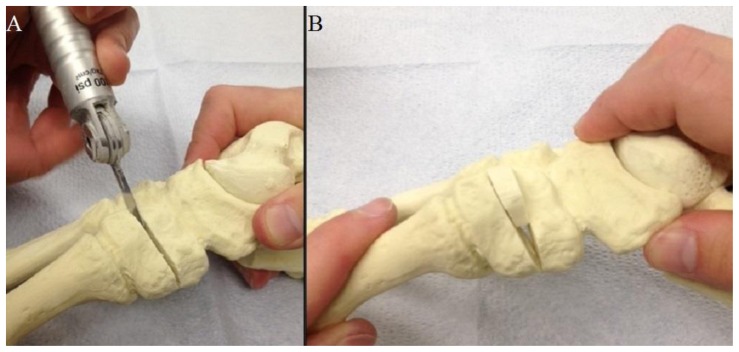
This pictorial review focuses on basic procedures performed within the field of podiatric surgery, specifically for elective reconstruction of the midfoot and rearfoot with focus on the flatfoot deformity. Our goal is to demonstrate objective radiographic parameters that surgeons utilize to initially define the deformity, lead to procedure selection, and judge post-operative outcomes. We hope that radiologists will employ this information to improve their assessment of post-operative radiographs following reconstructive foot surgeries. First, relevant radiographic measurements are defined and their role in procedure selection explained. Second, the specific surgical procedures of the Evans calcaneal osteotomy, medial calcaneal slide osteotomy, Cotton osteotomy, subtalar joint arthroeresis, and arthrodeses of the rearfoot are described. Finally, specific plain film radiographic findings that judge post-operative outcomes for each procedure are detailed.
Keywords: Calcaneal Osteotomy; Coalition; Cotton osteotomy; Flatfoot; Podiatric surgery.
Figures










References
-
- Mahan KT, Flanigan KP. Pes plano valgus deformity. In: Banks AS, Downey MS, Martin DE, Miller SJ, editors. McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. Third edition. Philadelphia: Lippincott, Williams and Wilkins; 2001. pp. 799–861. ASIN: B008GE9GEI.
-
- Dimmick S, Chhabra A, Grujic L, Linklater JM. Acquired flat foot deformity: Postoperative imaging. Semin Musculoskelet Radiol. 2012;16:217–232. - PubMed
-
- Sanner WH. Foot segmental relationships and bone morphology. In: Christman RA, editor. Foot and Ankle Radiology. First edition. ISBN-13. St Louis: Churchill Livingstone; 2003. pp. 272–302.pp. 978–0443087820.
-
- Meyr AJ, Wagoner MR. Descriptive quantitative analysis of rearfoot alignment radiographic parameters. J Foot Ankle Surg. 2015;54(5):860–71. - PubMed
-
- Williamson ERC, Chan JY, Burket JC, Deland JT, Ellis SJ. New radiographic parameter assessing hindfoot alignment in stage II adult-acquired flatfoot deformity. Foot Ankle Int. 2014;36(4):417–423. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical