

Paravertebral calcification as a potential indicator for nonaccidental trauma
- PMID: 29299097
- PMCID: PMC5743150
- DOI: 10.3941/jrcr.v11i7.2905
Paravertebral calcification as a potential indicator for nonaccidental trauma
Abstract
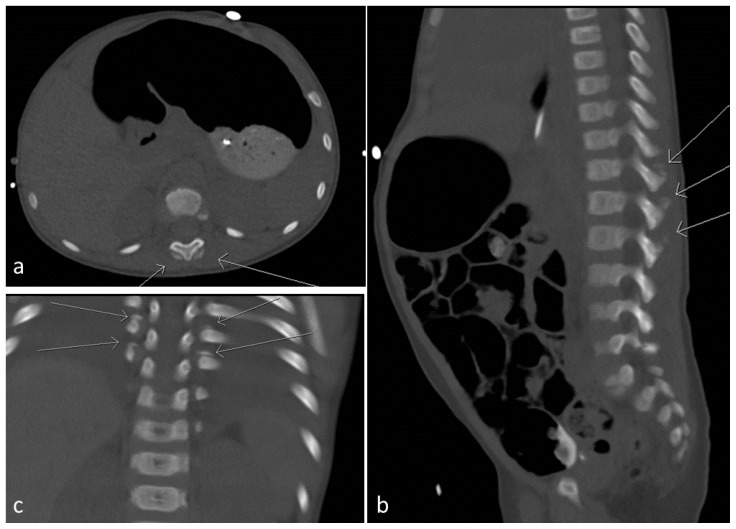
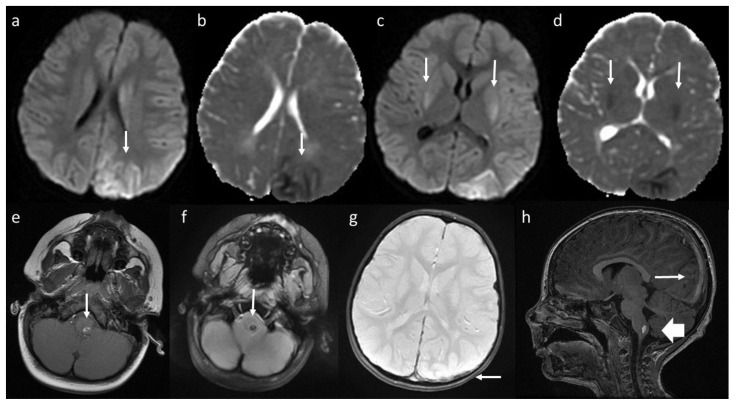
We report a case of nonaccidental trauma (NAT) involving a 23-month-old boy who presented with seizures, acute subarachnoid hemorrhage, and acute subdural hemorrhage. Ophthalmologic examination showed bilateral intraretinal hemorrhages. Further evaluation revealed that he had bilateral thoracolumbar paravertebral calcifications. The Children's Protective Services agency was involved in the case. The child was discharged to an inpatient rehabilitation facility. Vertebral fracture associated with paravertebral calcification has been reported as a sign of NAT. This case was unique because our patient had paravertebral calcifications without vertebral fracture. Paravertebral calcification alone could serve as an indicator of NAT.
Keywords: child abuse; paravertebral calcification; seizure; subarachnoid hemorrhage; subdural hemorrhage.
Figures

References
-
- Roaten JB, Partrick DA, Nydam TL, et al. Nonaccidental trauma is a major cause of morbidity and mortality among patients at a regional level 1 pediatric trauma center. Journal of pediatric surgery. 2006;41:2013–2015. - PubMed
-
- Lindberg DM, Beaty B, Juarez-Colunga E, et al. Pediatrics. 2015;136:831–838. - PubMed
-
- Levin TL, Berdon WE, Cassell I, et al. Pediatr Radiol. 2003;33:305–310. - PubMed
-
- Carrion WV, Dormans JP, Drummond DS, et al. Journal of pediatric orthopedics. 1996;16:210–214. - PubMed
-
- King WK, Kiesel EL, Simon HK. Child abuse fatalities: are we missing opportunities for intervention? Pediatric emergency care. 2006;22:211–214. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources