

The Radiologic and Pathologic Diagnosis of Biphasic Pulmonary Blastoma
- PMID: 29299105
- PMCID: PMC5743140
- DOI: 10.3941/jrcr.v11i9.3153
The Radiologic and Pathologic Diagnosis of Biphasic Pulmonary Blastoma
Abstract
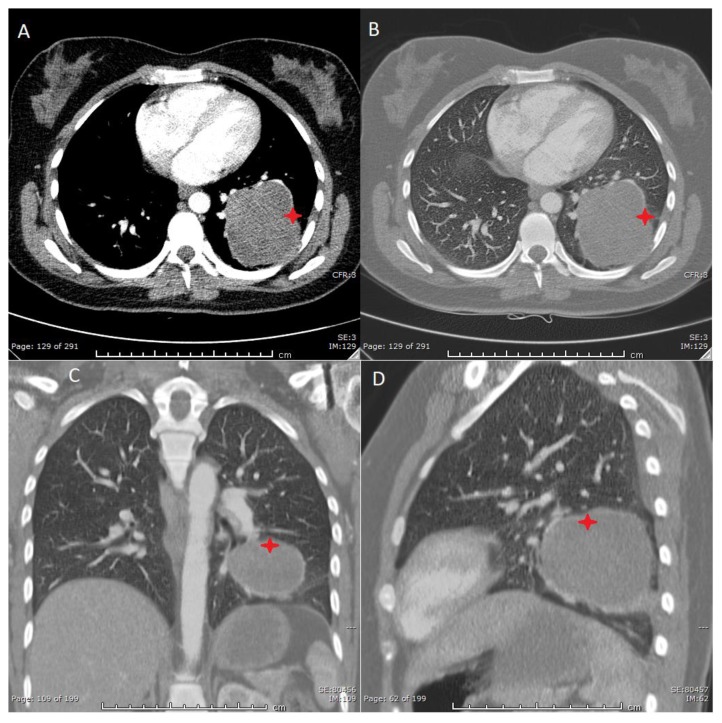
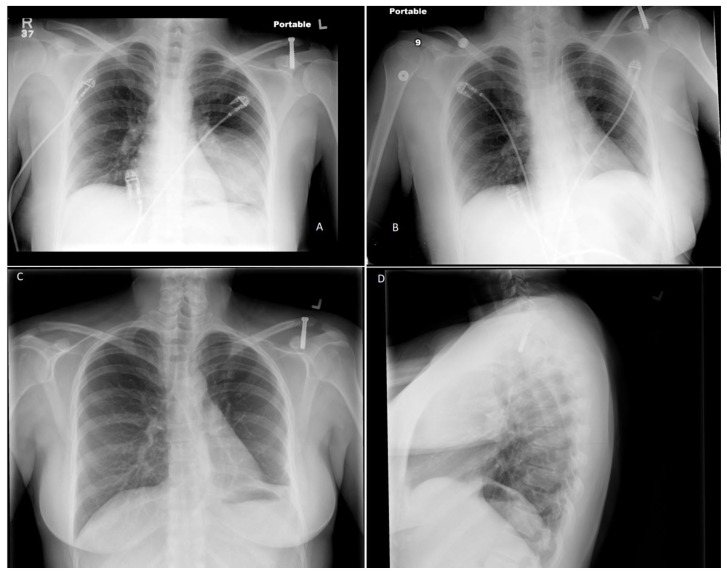
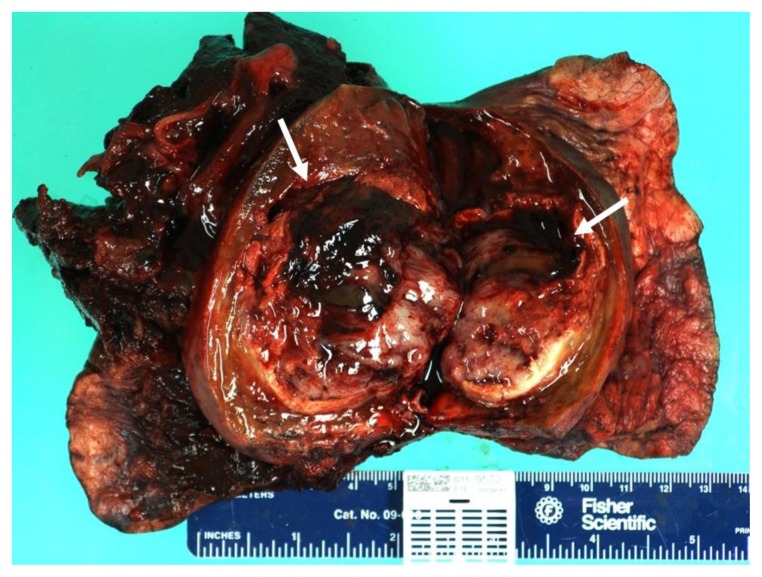
Pulmonary blastomas are rare malignancies, representing 0.25% to 0.5% of all primary lung neoplasms with often aggressive progression and poor prognosis. Clinical management of pulmonary blastomas depends on histologic subtype, staging, and presentation, and may consist of surgery, chemotherapy, and radiation. Biphasic pulmonary blastoma is a subtype of pulmonary blastoma that exhibits biphasic histology, with both epithelial and mesenchymal malignant elements. We report a case of biphasic pulmonary blastoma in a 33-year-old female with 1 pack per day history of smoking for approximately 16 years, who presented with left-sided pleuritic chest pain on deep inspiration without otherwise significant pat medical history. Imaging evaluation using chest radiography, computed tomography, and magnetic resonance imaging identified a heterogenous, well-circumscribed, left lower lobe mass with extensive necrosis and hemorrhage. No lymphadenopathy or distant metastasis was detected through imaging evaluation. Surgical resection of the tumor followed by histopathological analysis confirmed a biphasic pulmonary blastoma.
Keywords: Biphasic Pulmonary Blastoma; Computed Tomography; Magnetic Resonance Imaging; Pulmonary Blastoma; Pulmonary Neoplasm.
Figures





Similar articles
-
Survival of biphasic pulmonary blastoma.Respir Med. 2006 Jul;100(7):1174-9. doi: 10.1016/j.rmed.2005.10.026. Epub 2005 Dec 5. Respir Med. 2006. PMID: 16332433
-
[Pulmonary blastoma--a rare malignant lung tumor].Chirurg. 2001 Jan;72(1):86-8. doi: 10.1007/s001040051273. Chirurg. 2001. PMID: 11225463 German.
-
Radical resection of a pulmonary blastoma involving the pulmonary artery.Eur J Cardiothorac Surg. 2008 Sep;34(3):695-6. doi: 10.1016/j.ejcts.2008.05.020. Epub 2008 Jun 25. Eur J Cardiothorac Surg. 2008. PMID: 18579394
-
[Pleuropulmonary blastoma: a case report].Tuberk Toraks. 2003;51(4):436-9. Tuberk Toraks. 2003. PMID: 15143394 Review. Turkish.
-
Pulmonary blastoma: a case report and review of the literature.BMC Res Notes. 2014 May 13;7:294. doi: 10.1186/1756-0500-7-294. BMC Res Notes. 2014. PMID: 24885892 Free PMC article. Review.
Cited by
-
Characteristics and clinical outcomes of pulmonary sarcomatoid carcinoma: experience from Tata Memorial Centre.Ecancermedicalscience. 2022 Aug 8;16:1438. doi: 10.3332/ecancer.2022.1438. eCollection 2022. Ecancermedicalscience. 2022. PMID: 36200011 Free PMC article.
-
Pulmonary blastoma with a good prognosis: a case report and review of the literature.J Int Med Res. 2024 Jun;52(6):3000605241254778. doi: 10.1177/03000605241254778. J Int Med Res. 2024. PMID: 38835107 Free PMC article. Review.
-
Classic biphasic pulmonary blastoma with endobronchial invasion in a 16-year-old male: A rare case report.Respir Med Case Rep. 2024 Nov 19;52:102143. doi: 10.1016/j.rmcr.2024.102143. eCollection 2024. Respir Med Case Rep. 2024. PMID: 39654606 Free PMC article.
-
Pleuropulmonary blastoma, a rare entity in childhood.BJR Case Rep. 2021 Apr 29;7(4):20200206. doi: 10.1259/bjrcr.20200206. eCollection 2021 Jul 16. BJR Case Rep. 2021. PMID: 35047198 Free PMC article.
-
Classic biphasic pulmonary blastoma: A case report and review of the literature from 2000 to 2022.Clin Respir J. 2023 Nov;17(11):1103-1116. doi: 10.1111/crj.13701. Epub 2023 Sep 29. Clin Respir J. 2023. PMID: 37772674 Free PMC article. Review.
References
-
- Francis D, Jacobsen M. Pulmonary Diseases. Springer; 1983. Pulmonary blastoma; pp. 265–94. - PubMed
-
- Spencer H. Pulmonary blastomas. J Pathol. 1961;82(1):161–6.
-
- Berean K, Truong LD, Dudley AW, Jr, Cagle PT. Immunohistochemical characterization of pulmonary blastoma. Am J Clin Pathol. 1988;89(6):773–7. - PubMed
-
- Sharma A, O’Gorman K, Aman C, Rassl D, Mohamid W, Polychronis A. A rare occurrence of biphasic pulmonary blastoma in an elderly male. Anticancer Res. 2013;33(9):3911–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical