

Specimen mapping in head and neck cancer using fluorescence imaging
- PMID: 29299522
- PMCID: PMC5743163
- DOI: 10.1002/lio2.84
Specimen mapping in head and neck cancer using fluorescence imaging
Abstract
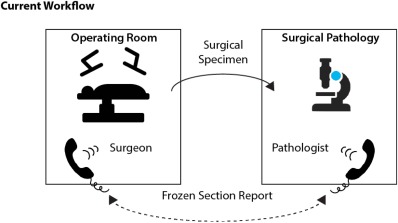
Overview: Although the agreed-upon standard is circumferential pathology analysis of the interface between the resected specimen and the patient, there is currently no consensus on the optimal methodology to achieve this in head and neck cancer specimens. This is most commonly conducted by either sampling the wound bed after resection or obtaining samples from the specimen. Regardless of the technique, only a fraction of the area of interest can be sampled due to the labor-intensive nature of frozen sections.
Objective: This review will cover and define the possible role for optical mapping of the surgical specimen using fluorescence imaging in head and neck cancer.
Level of evidence: NA.
Keywords: Surgery; fluorescence; image‐guidance; oncology; probes.
Figures

References
-
- McMahon J, O'Brien CJ, Pathak I, et al. Influence of condition of surgical margins on local recurrence and disease‐specific survival in oral and oropharyngeal cancer. Br J Oral Maxillofac Surg 2003;41:224–231. - PubMed
-
- Woolgar JA, Triantafyllou A. Pitfalls and procedures in the histopathological diagnosis of oral and oropharyngeal squamous cell carcinoma and a review of the role of pathology in prognosis. Oral Oncol 2009;45:361–385. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials