

The Key Roles of Negative Pressure Breathing and Exercise in the Development of Interstitial Pulmonary Edema in Professional Male SCUBA Divers
- PMID: 29299780
- PMCID: PMC5752643
- DOI: 10.1186/s40798-017-0116-x
The Key Roles of Negative Pressure Breathing and Exercise in the Development of Interstitial Pulmonary Edema in Professional Male SCUBA Divers
Abstract
Background: Immersion pulmonary edema is potentially a catastrophic condition; however, the pathophysiological mechanisms are ill-defined. This study assessed the individual and combined effects of exertion and negative pressure breathing on the cardiovascular system during the development of pulmonary edema in SCUBA divers.
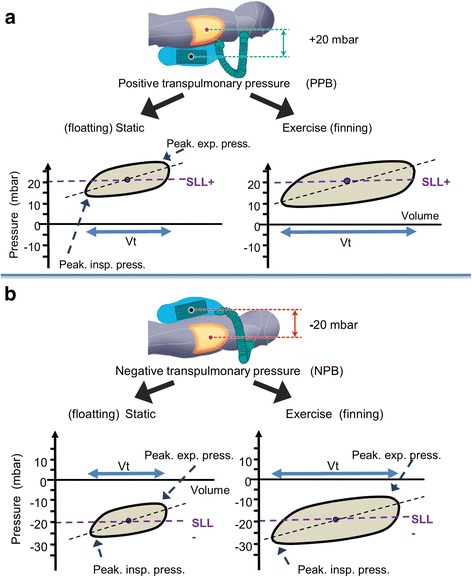
Methods: Sixteen male professional SCUBA divers performed four SCUBA dives in a freshwater pool at 1 m depth while breathing air at either a positive or negative pressure both at rest or with exercise. Echocardiography and lung ultrasound were used to assess the cardiovascular changes and lung comet score (a measure of interstitial pulmonary edema).
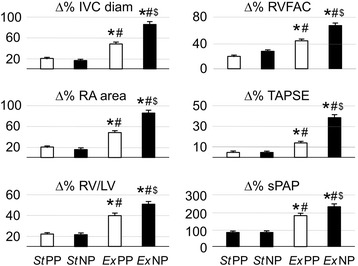
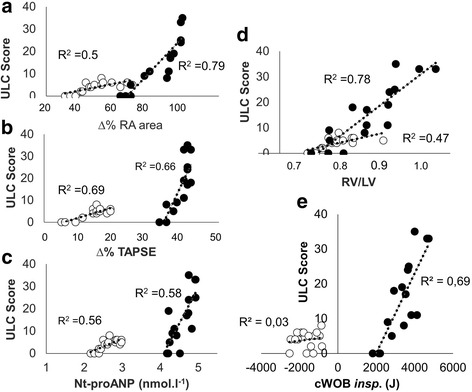
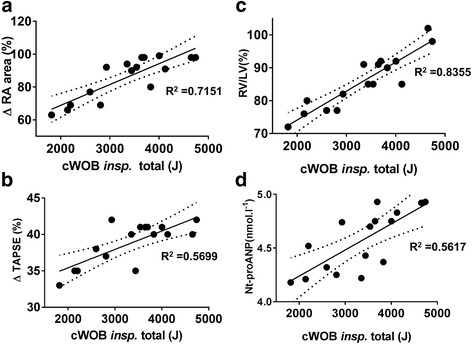
Results: The ultrasound lung comet score was 0 following both the dives at rest regardless of breathing pressure. Following exercise, the mean comet score rose to 4.2 with positive pressure breathing and increased to 15.1 with negative pressure breathing. The development of interstitial pulmonary edema was significantly related to inferior vena cava diameter, right atrial area, tricuspid annular plane systolic excursion, right ventricular fractional area change, and pulmonary artery pressure. Exercise combined with negative pressure breathing induced the greatest changes in these cardiovascular indices and lung comet score.
Conclusions: A diver using negative pressure breathing while exercising is at greatest risk of developing interstitial pulmonary edema. The development of immersion pulmonary edema is closely related to hemodynamic changes in the right but not the left ventricle. Our findings have important implications for divers and understanding the mechanisms of pulmonary edema in other clinical settings.
Keywords: Atrial natriuretic peptide; Echocardiography; Exercise; Hydrostatic transrespiratory pressure; Immersion pulmonary edema; Inspiratory breathing effort; Lung ultrasonography; Negative pressure breathing; Right heart preload; Work of breathing.
Conflict of interest statement
Authors’ Information
Not applicable
Ethics Approval and Consent to Participate
All experimental procedures were conducted in line with the Declaration of Helsinki, and the study protocol was approved by the local Ethics Committee (Comité de Protection des Personnes-CPP Sud Méditerranée V, ref. 16.077).
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
Not applicable
Competing Interests
Olivier Castagna, Jacques Regnard, Emmanuel Gempp, Pierre Louge, François-Xavier Brocq, Bruno Schmid, Anne-Virginie Desruelle, Valentin Crunel, Adrien Maurin, Romain Chopard, and David MacIver declare that they have no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Cardiovascular Mechanisms of Extravascular Lung Water Accumulation in Divers.Am J Cardiol. 2017 Mar 15;119(6):929-932. doi: 10.1016/j.amjcard.2016.11.050. Epub 2017 Jan 20. Am J Cardiol. 2017. PMID: 28189252
-
Assessment of extravascular lung water and cardiac function in trimix SCUBA diving.Med Sci Sports Exerc. 2010 Jun;42(6):1054-61. doi: 10.1249/MSS.0b013e3181c5b8a8. Med Sci Sports Exerc. 2010. PMID: 19997032
-
Pulmonary Aspects of Exercise and Sports.Methodist Debakey Cardiovasc J. 2016 Apr-Jun;12(2):93-7. doi: 10.14797/mdcj-12-2-93. Methodist Debakey Cardiovasc J. 2016. PMID: 27486491 Free PMC article. Review.
-
Immersion pulmonary oedema in a healthy diver not exposed to cold or strenuous exercise.Diving Hyperb Med. 2018 Mar 31;48(1):40-44. doi: 10.28920/dhm48.1.40-44. Diving Hyperb Med. 2018. PMID: 29557101 Free PMC article.
-
Pulmonary edema associated with scuba diving : case reports and review.Chest. 2001 Nov;120(5):1686-94. doi: 10.1378/chest.120.5.1686. Chest. 2001. PMID: 11713154 Review.
Cited by
-
Pulmonary Effects of One Week of Repeated Recreational Closed-Circuit Rebreather Dives in Cold Water.Medicina (Kaunas). 2022 Dec 30;59(1):81. doi: 10.3390/medicina59010081. Medicina (Kaunas). 2022. PMID: 36676705 Free PMC article.
-
Medical conditions that affect the risk of diving.BJA Educ. 2021 Sep;21(9):349-354. doi: 10.1016/j.bjae.2021.05.002. Epub 2021 Jul 13. BJA Educ. 2021. PMID: 34457355 Free PMC article. Review. No abstract available.
-
Continuous humidification enhances postoperative recovery in laryngeal cancer patients undergoing tracheotomy.Am J Transl Res. 2021 Nov 15;13(11):12852-12859. eCollection 2021. Am J Transl Res. 2021. PMID: 34956500 Free PMC article.
-
Snorkelling and Breath-Hold Diving Fatalities in Australia-A Review of 317 Deaths.Int J Environ Res Public Health. 2025 Jan 18;22(1):119. doi: 10.3390/ijerph22010119. Int J Environ Res Public Health. 2025. PMID: 39857572 Free PMC article. Review.
-
Joint position statement on immersion pulmonary oedema and diving from the South Pacific Underwater Medicine Society (SPUMS) and the United Kingdom Diving Medical Committee (UKDMC) 2024.Diving Hyperb Med. 2024 Dec 20;54(4):344-349. doi: 10.28920/dhm54.4.344-349. Diving Hyperb Med. 2024. PMID: 39675743 Free PMC article.
References
-
- Pons M, Blickenstorfer D, Oechslin E, Hold G, Greminger P, Franzeck UK, et al. Pulmonary oedema in healthy persons during scuba-diving and swimming. Eur Respir J. 1995;8(5):762–767. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
