Role of Penile Prosthesis in Priapism: A Review
- PMID: 29299902
- PMCID: PMC5756805
- DOI: 10.5534/wjmh.17040
Role of Penile Prosthesis in Priapism: A Review
Abstract
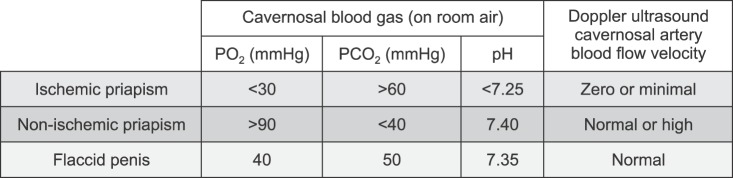
Ischemic priapism is a urological emergency that has been associated with long-standing and irreversible adverse effects on erectile function. Studies have demonstrated a linear relationship between the duration of critically ischemic episodes and the subsequent development of corporal fibrosis and irreversible erectile function loss. Placement of a penile prosthesis is a well-established therapeutic option for the management of erectile dysfunction secondary to ischemic priapism, and will be the focus of this review. Review of the current literature demonstrates a growing utilization of penile prostheses in the treatment of erectile dysfunction secondary to ischemic priapism. Unfortunately, there is a paucity of randomized-controlled trials describing the use of prosthesis in ischemic priapism. As a result, there is a lack of consensus regarding the type of prosthesis (malleable vs. inflatable), timing of surgery (acute vs. delayed), and anticipated complications for each approach. Both types of prostheses yielded comparable complication rates, but the inflatable penile prosthesis have higher satisfaction rates. Acute treatment of priapism was associated with increased risk of prosthetic infection, and could potentially cause psychological trauma, whereas delayed implantation was associated with greater corporal fibrosis, loss of penile length, and increased technical difficulty of implantation. The paucity of high-level evidence fuels the ongoing discussion of optimal use and timing of penile prosthesis implantation. Current guidance is based on consensus expert opinion derived from small, retrospective studies. Until more robust data is available, a patient-centered approach and joint decision-making between the patient and his urologist is recommended.
Keywords: Erectile dysfunction; Priapism; Prostheses and implants.
Copyright © 2018 Korean Society for Sexual Medicine and Andrology.
Conflict of interest statement
Dr. Wayne J.G. Hellstrom is an adviser for Coloplast (Minneapolis, MN, USA) and Boston Scientific (Marlborough, PA, USA), but this has made no influence on this work in relation with the company or its products. Other authors have no potential conflicts of interest to disclose.
Figures
References
-
- Montague DK, Jarow J, Broderick GA, Dmochowski RR, Heaton JP, Lue TF, et al. American Urological Association guideline on the management of priapism. J Urol. 2003;170:1318–1324. - PubMed
-
- Eland IA, van der Lei J, Stricker BH, Sturkenboom MJ. Incidence of priapism in the general population. Urology. 2001;57:970–972. - PubMed
-
- Kadioglu A, Sanli O, Celtik M, Cakan M, Taskapu H, Akman T. Practical management of patients with priapism. EAU-EBU Update Ser. 2006;4:150–160.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials