

Contemporary Risk Factors and Outcomes of Transfusion-Associated Circulatory Overload
- PMID: 29300236
- PMCID: PMC5851817
- DOI: 10.1097/CCM.0000000000002948
Contemporary Risk Factors and Outcomes of Transfusion-Associated Circulatory Overload
Abstract
Objectives: Transfusion-associated circulatory overload is characterized by hydrostatic pulmonary edema following blood transfusion. Restrictive transfusion practice may affect the occurrence and severity of transfusion-associated circulatory overload in critically ill patients. We sought to examine contemporary risk factors and outcomes for transfusion-associated circulatory overload.
Design: Case-control study.
Setting: Four tertiary care hospitals.
Patients: We prospectively enrolled 200 patients with transfusion-associated circulatory overload identified by active surveillance and 405 controls matched by transfusion intensity.
Interventions: None.
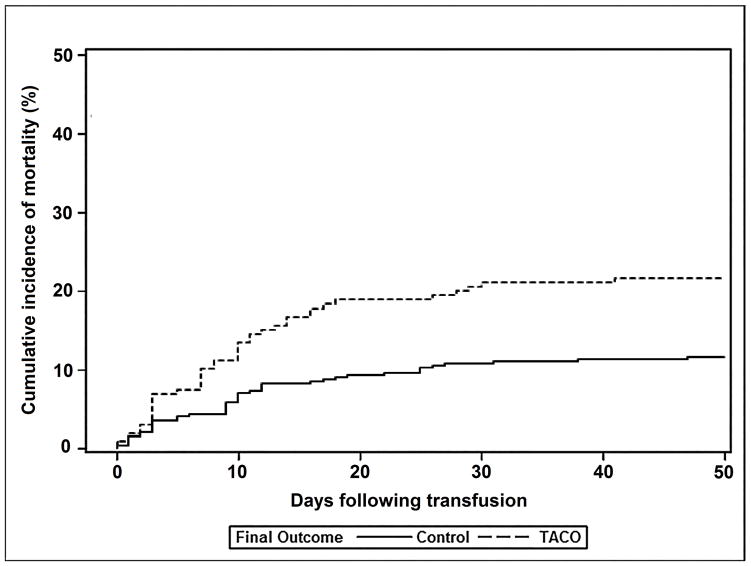
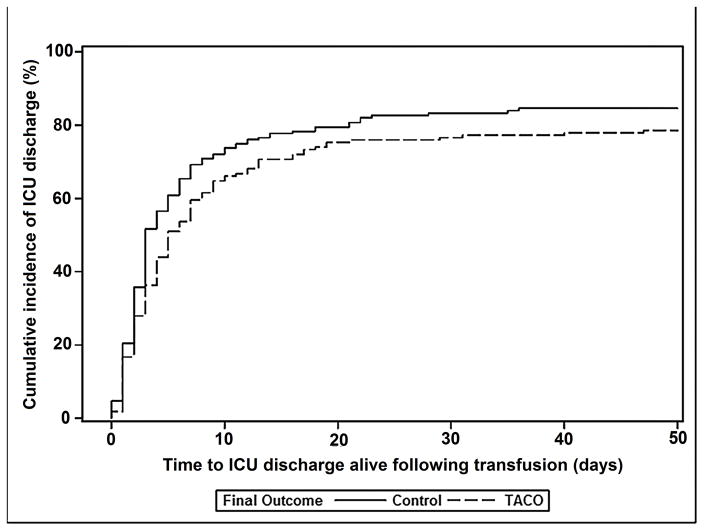
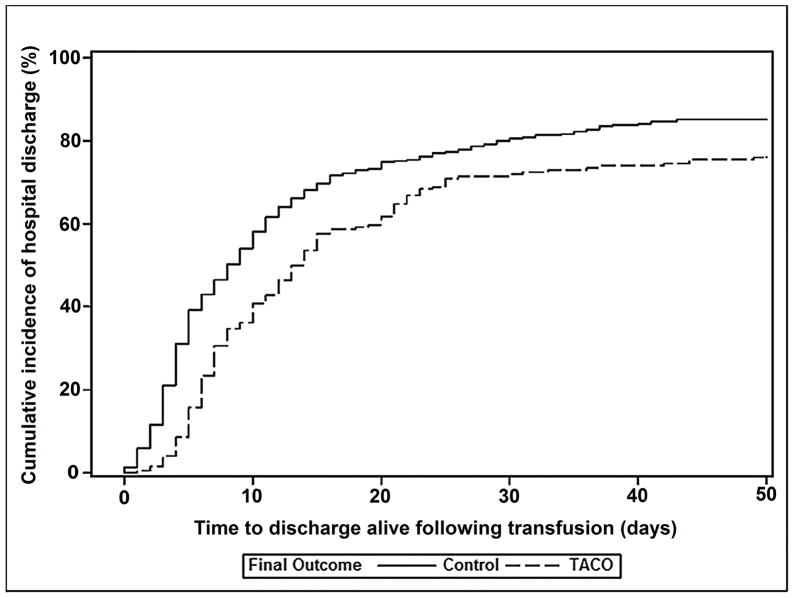
Measurements and main results: Among 20,845 transfused patients who received 128,263 blood components from May 2015 until July 2016, transfusion-associated circulatory overload incidence was one case per 100 transfused patients. In addition to cardiovascular comorbidities, multivariable analysis identified the following independent predictors of transfusion-associated circulatory overload: acute kidney injury, emergency surgery, pretransfusion diuretic use, and plasma transfusion-the latter especially in females. Compared with matched controls, transfusion-associated circulatory overload cases were more likely to require mechanical ventilation (71% vs 49%; p < 0.001), experienced longer intensive care and hospital lengths of stay following transfusion, and had higher mortality (21% vs 11%; p = 0.02) even after adjustment for other potentially confounding variables.
Conclusions: Despite restrictive transfusion practice, transfusion-associated circulatory overload remains a frequent complication of transfusion and is an independent risk factor for in-hospital morbidity and mortality. In addition to cardiovascular and renal risk factors, plasma transfusion was associated with transfusion-associated circulatory overload after controlling for other covariates. Additional research is needed to examine the benefit of reduced erythrocyte or plasma exposure in patients at high risk for transfusion-associated circulatory overload.
Figures
Comment in
-
The First Steps in Understanding of Transfusion-Associated Circulatory Overload-We Are on a "Roll".Crit Care Med. 2018 Apr;46(4):650-651. doi: 10.1097/CCM.0000000000002971. Crit Care Med. 2018. PMID: 29538118 No abstract available.
References
-
- Waters JH, Ness PM. Patient blood management: a growing challenge and opportunity. Transfusion. 2011;51(5):902–903. - PubMed
-
- Goodnough LT, Shah N. The next chapter in patient blood management: real-time clinical decision support. Am J Clin Pathol. 2014;142(6):741–747. - PubMed
-
- Oliver JC, Griffin RL, Hannon T, et al. The success of our patient blood management program depended on an institution-wide change in transfusion practices. Transfusion. 2014;54(10 Pt 2):2617–2624. - PubMed
-
- Collins RA, Wisniewski MK, Waters JH, et al. Effectiveness of multiple initiatives to reduce blood component wastage. Am J Clin Pathol. 2015;143(3):329–335. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- L30 HL129355/HL/NHLBI NIH HHS/United States
- HHSN268201100003C/WH/WHI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100002C/WH/WHI NIH HHS/United States
- HHSN268201000003C/HL/NHLBI NIH HHS/United States
- HHSN268201000004C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100003I/HL/NHLBI NIH HHS/United States
- HHSN268201100002I/HL/NHLBI NIH HHS/United States
- HHSN268201000002C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100004I/HL/NHLBI NIH HHS/United States
- HHSN268201100004C/WH/WHI NIH HHS/United States
- HHSN268201000005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
