

Adaptation and validation of the ACMG/AMP variant classification framework for MYH7-associated inherited cardiomyopathies: recommendations by ClinGen's Inherited Cardiomyopathy Expert Panel
- PMID: 29300372
- PMCID: PMC5876064
- DOI: 10.1038/gim.2017.218
Adaptation and validation of the ACMG/AMP variant classification framework for MYH7-associated inherited cardiomyopathies: recommendations by ClinGen's Inherited Cardiomyopathy Expert Panel
Abstract
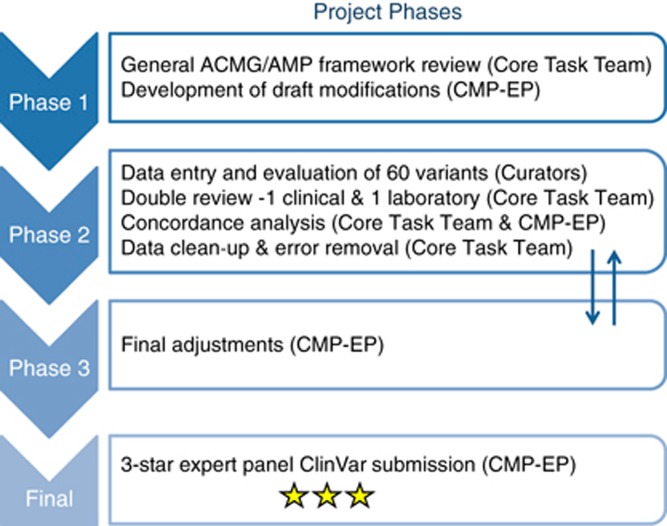
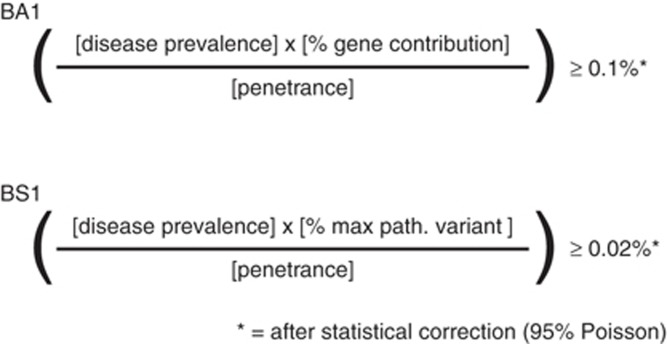
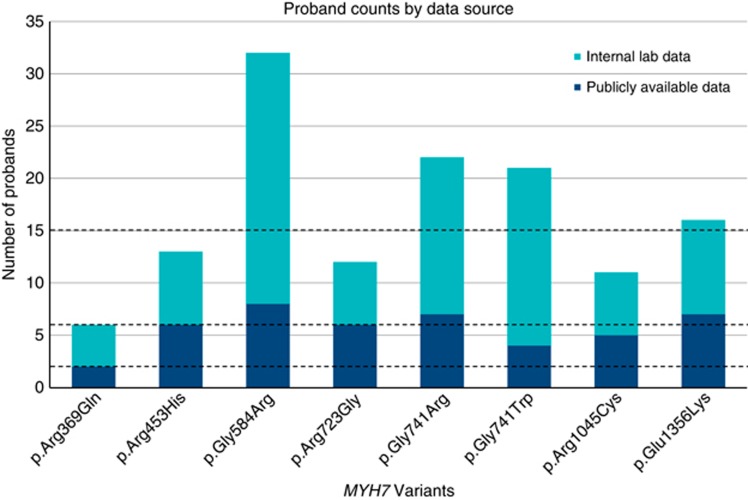
PurposeIntegrating genomic sequencing in clinical care requires standardization of variant interpretation practices. The Clinical Genome Resource has established expert panels to adapt the American College of Medical Genetics and Genomics/Association for Molecular Pathology classification framework for specific genes and diseases. The Cardiomyopathy Expert Panel selected MYH7, a key contributor to inherited cardiomyopathies, as a pilot gene to develop a broadly applicable approach.MethodsExpert revisions were tested with 60 variants using a structured double review by pairs of clinical and diagnostic laboratory experts. Final consensus rules were established via iterative discussions.ResultsAdjustments represented disease-/gene-informed specifications (12) or strength adjustments of existing rules (5). Nine rules were deemed not applicable. Key specifications included quantitative frameworks for minor allele frequency thresholds, the use of segregation data, and a semiquantitative approach to counting multiple independent variant occurrences where fully controlled case-control studies are lacking. Initial inter-expert classification concordance was 93%. Internal data from participating diagnostic laboratories changed the classification of 20% of the variants (n = 12), highlighting the critical importance of data sharing.ConclusionThese adapted rules provide increased specificity for use in MYH7-associated disorders in combination with expert review and clinical judgment and serve as a stepping stone for genes and disorders with similar genetic and clinical characteristics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pepin MG, Murray ML, Bailey S, Leistritz-Kessler D, Schwarze U, Byers PH. The challenge of comprehensive and consistent sequence variant interpretation between clinical laboratories. Genet Med. 2016;18:20–24. - PubMed
-
- Gaba P, Bos JM, Cannon BC et al. Implantable cardioverter-defibrillator explantation for overdiagnosed or overtreated congenital long QT syndrome. Heart Rhythm. 2016;13:879–885. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_U120085815/MRC_/Medical Research Council/United Kingdom
- U41 HG006834/HG/NHGRI NIH HHS/United States
- U41 HG009649/HG/NHGRI NIH HHS/United States
- RG/12/16/29939/BHF_/British Heart Foundation/United Kingdom
- U01 HG007437/HG/NHGRI NIH HHS/United States
- NIHR-HCS-D13-04-006/DH_/Department of Health/United Kingdom
- SP/10/10/28431/BHF_/British Heart Foundation/United Kingdom
- MC_UP_1102/20/MRC_/Medical Research Council/United Kingdom
- 107469/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- U41 HG009650/HG/NHGRI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
