

Which factor is the most effective one in metabolic Sydrome on the outcomes after coronary artery bypass graft surgery? A cohort study of 5 Years
- PMID: 29301583
- PMCID: PMC5753490
- DOI: 10.1186/s13019-017-0682-5
Which factor is the most effective one in metabolic Sydrome on the outcomes after coronary artery bypass graft surgery? A cohort study of 5 Years
Abstract
Background: Metabolic Syndrome and diabetes mellitus are risk factors for cardiovascular disease. However, the effects of Metabolic Syndrome with or without diabetes on perioperative and long-term morbidity and mortality after Coronary Artery Bypass Graft remain unclear.
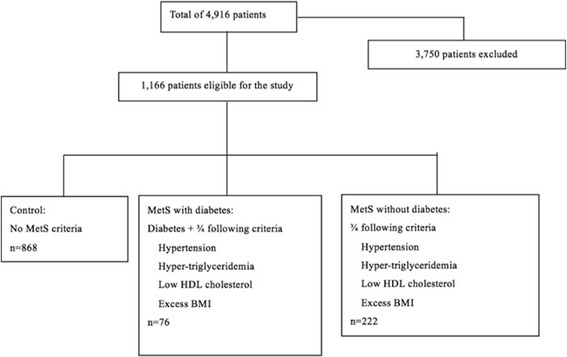
Methods: An retrospective study was performed on 1166 patients who received isolated primary Coronary Artery Bypass Graft in Fuwai hospital. They were divided into three groups: control, Metabolic Syndrome of three factors together with diabetes and Metabolic Syndrome of three factors without diabetes (n = 868, 76 and 222 respectively). Analysis of variance, Chi-rank test, Fisher's exact test, Log-rank test, Cox and Logistic regression models were used for data processing. Outcomes were postoperative and 5-year survival and morbidities.
Results: There were no significant differences between groups in in-hospital postoperative complications, epinephrine use, stroke, atrial fibrillation, renal failure, coma, myocardial infarction and repeated revascularization. Patients in the Metabolic Syndrome with diabetes, Metabolic Syndrome without diabetes and control groups, respectively, showed significant difference in perioperative Major Adverse Cerebral Cardiovascular Events (30.3% vs. 21.2%, 16.7%, P = 0.0071) and mortality (11.8% vs. 2.7%, 3.11%, P = 0.0003). The Metabolic Syndrome with diabetes group had higher rates of perioperative mortality than Metabolic Syndrome without diabetes (P = 0.0017, P of Fisher Test = 0.0039). Compared with non-diabetic patients with Metabolic Syndrome, those with Metabolic Syndrome and diabetes had increased long-term mortality (Adjusted HR: 4.3; 95% CI: 1.4-13.3; P = 0.0113) and Major Adverse Cerebral Cardiovascular Events (Adjusted OR: 1.7; 95% CI: 1.0-2.8; P = 0.048). Control and non-diabetic Metabolic Syndrome groups did not differ in long-term mortality but controls had lower rates of Major Adverse Cerebral Cardiovascular Events (Adjusted OR: 0.79; 95% CI: 0.64-0.98; P = 0.0329).
Conclusions: There were significance differences between the three groups in perioperative Major Adverse Cerebral Cardiovascular Events and mortality after Coronary Artery Bypass Graft. Compared with non-diabetic Metabolic Syndrome patients, patients with Metabolic Syndrome and diabetes had higher long-term Major Adverse Cerebral Cardiovascular Events and mortality. While patients free of MetS and diabetes were associated with lower incidence of long-term Major Adverse Cerebral Cardiovascular Events after Coronary Artery Bypass Graft.
Keywords: Coronary artery bypass graft surgery; Diabetes; Major adverse cerebral cardiovascular events; Metabolic syndrome.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted in accord with the Declaration of Helsinki principals and approved by the Fuwai Hospital Institutional Review Board. Informed consent (Consent to Participate) was obtained from each of the patients.
Consent for publication
Informed consent was obtained from the patient for publication of this report and available for review.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
