

Genomic correlates of response to immune checkpoint therapies in clear cell renal cell carcinoma
- PMID: 29301960
- PMCID: PMC6035749
- DOI: 10.1126/science.aan5951
Genomic correlates of response to immune checkpoint therapies in clear cell renal cell carcinoma
Abstract
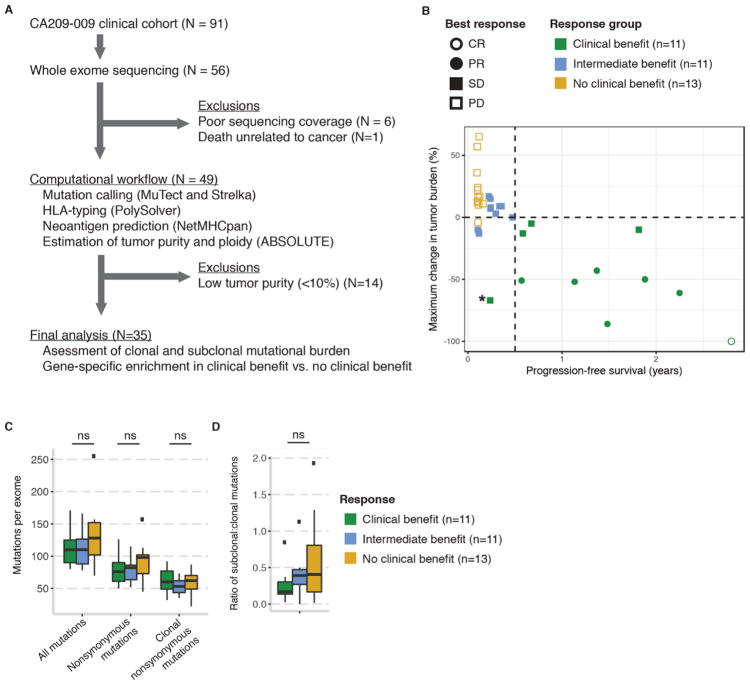
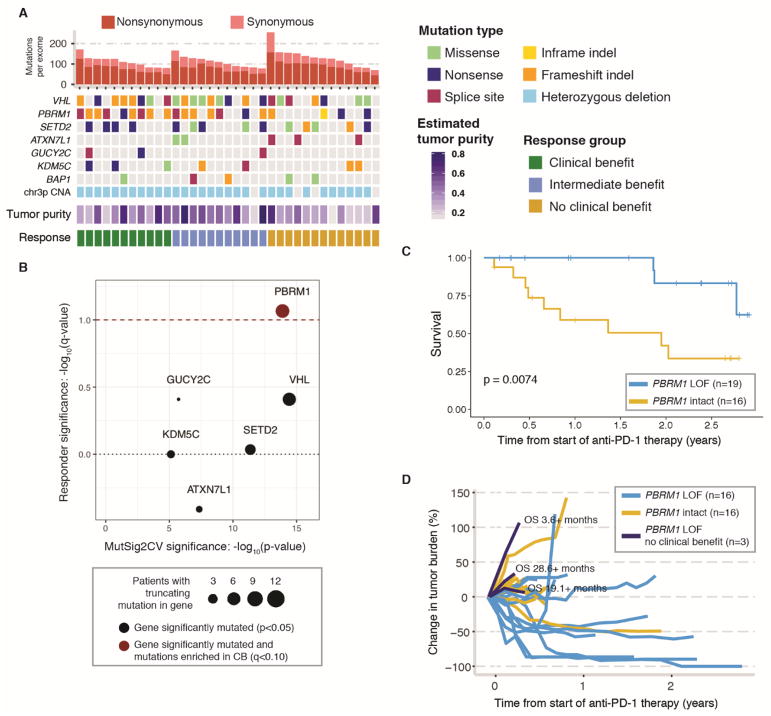
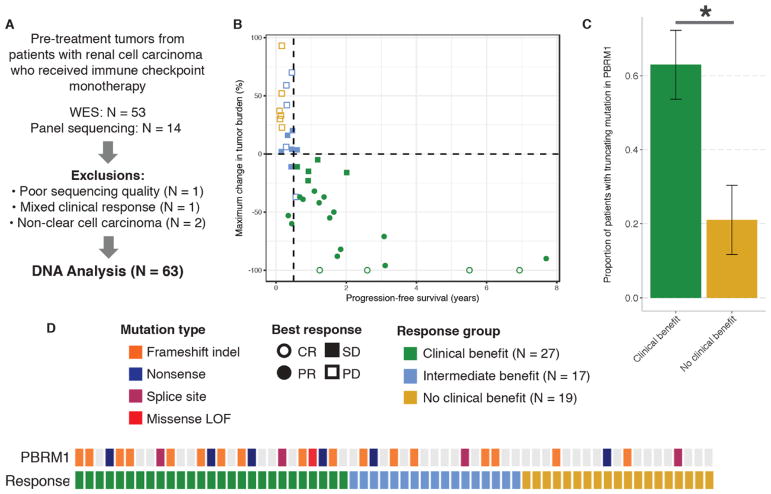
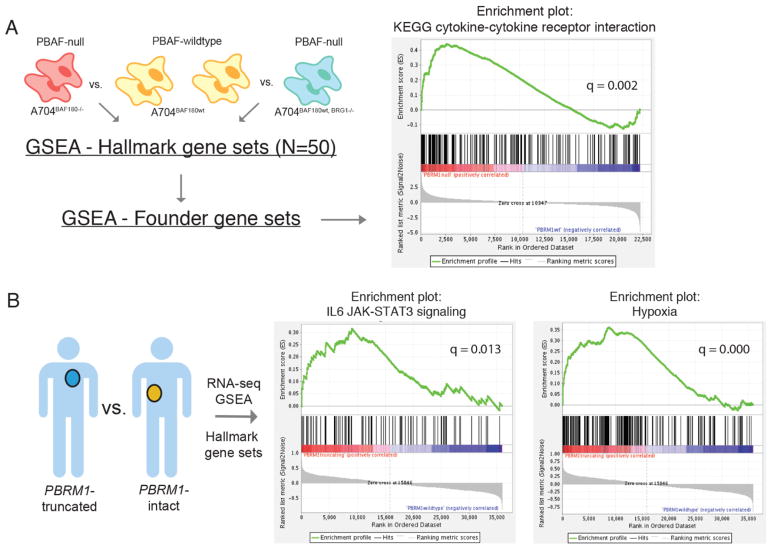
Immune checkpoint inhibitors targeting the programmed cell death 1 receptor (PD-1) improve survival in a subset of patients with clear cell renal cell carcinoma (ccRCC). To identify genomic alterations in ccRCC that correlate with response to anti-PD-1 monotherapy, we performed whole-exome sequencing of metastatic ccRCC from 35 patients. We found that clinical benefit was associated with loss-of-function mutations in the PBRM1 gene (P = 0.012), which encodes a subunit of the PBAF switch-sucrose nonfermentable (SWI/SNF) chromatin remodeling complex. We confirmed this finding in an independent validation cohort of 63 ccRCC patients treated with PD-1 or PD-L1 (PD-1 ligand) blockade therapy alone or in combination with anti-CTLA-4 (cytotoxic T lymphocyte-associated protein 4) therapies (P = 0.0071). Gene-expression analysis of PBAF-deficient ccRCC cell lines and PBRM1-deficient tumors revealed altered transcriptional output in JAK-STAT (Janus kinase-signal transducers and activators of transcription), hypoxia, and immune signaling pathways. PBRM1 loss in ccRCC may alter global tumor-cell expression profiles to influence responsiveness to immune checkpoint therapy.
Copyright © 2018 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Comment in
-
Kidney cancer: PBRM1 loss promotes tumour response to immunotherapy.Nat Rev Nephrol. 2018 Mar;14(3):142. doi: 10.1038/nrneph.2018.7. Epub 2018 Jan 22. Nat Rev Nephrol. 2018. PMID: 29355171 No abstract available.
-
Kidney cancer: PBRM1 loss promotes tumour response to immunotherapy.Nat Rev Clin Oncol. 2018 Mar;15(3):134-135. doi: 10.1038/nrclinonc.2018.12. Epub 2018 Jan 23. Nat Rev Clin Oncol. 2018. PMID: 29358781 No abstract available.
-
Chromatin regulation and immune escape.Science. 2018 Feb 16;359(6377):745-746. doi: 10.1126/science.aat0383. Science. 2018. PMID: 29449480 No abstract available.
References
-
- Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, Tykodi SS, Sosman JA, Procopio G, Plimack ER, Castellano D, Choueiri TK, Gurney H, Donskov F, Bono P, Wagstaff J, Gauler TC, Ueda T, Tomita Y, Schutz FA, Kollmannsberger C, Larkin J, Ravaud A, Simon JS, Xu LA, Waxman IM, Sharma P. CheckMate 025 Investigators, Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373:1803–1813. doi: 10.1056/NEJMoa1510665. - DOI - PMC - PubMed
-
- Snyder A, Makarov V, Merghoub T, Yuan J, Zaretsky JM, Desrichard A, Walsh LA, Postow MA, Wong P, Ho TS, Hollmann TJ, Bruggeman C, Kannan K, Li Y, Elipenahli C, Liu C, Harbison CT, Wang L, Ribas A, Wolchok JD, Chan TA. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N Engl J Med. 2014;371:2189–2199. doi: 10.1056/NEJMoa1406498. - DOI - PMC - PubMed
-
- Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, Lee W, Yuan J, Wong P, Ho TS, Miller ML, Rekhtman N, Moreira AL, Ibrahim F, Bruggeman C, Gasmi B, Zappasodi R, Maeda Y, Sander C, Garon EB, Merghoub T, Wolchok JD, Schumacher TN, Chan TA. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015;348:124–128. doi: 10.1126/science.aaa1348. - DOI - PMC - PubMed
-
- Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, Skora AD, Luber BS, Azad NS, Laheru D, Biedrzycki B, Donehower RC, Zaheer A, Fisher GA, Crocenzi TS, Lee JJ, Duffy SM, Goldberg RM, de la Chapelle A, Koshiji M, Bhaijee F, Huebner T, Hruban RH, Wood LD, Cuka N, Pardoll DM, Papadopoulos N, Kinzler KW, Zhou S, Cornish TC, Taube JM, Anders RA, Eshleman JR, Vogelstein B, Diaz LA., Jr PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015;372:2509–2520. doi: 10.1056/NEJMoa1500596. - DOI - PMC - PubMed
-
- Van Allen EM, Miao D, Schilling B, Shukla SA, Blank C, Zimmer L, Sucker A, Hillen U, Foppen MHG, Goldinger SM, Utikal J, Hassel JC, Weide B, Kaehler KC, Loquai C, Mohr P, Gutzmer R, Dummer R, Gabriel S, Wu CJ, Schadendorf D, Garraway LA. Genomic correlates of response to CTLA-4 blockade in metastatic melanoma. Science. 2015;350:207–211. doi: 10.1126/science.aad0095. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
