

Biomaterial-driven in situ cardiovascular tissue engineering-a multi-disciplinary perspective
- PMID: 29302354
- PMCID: PMC5677971
- DOI: 10.1038/s41536-017-0023-2
Biomaterial-driven in situ cardiovascular tissue engineering-a multi-disciplinary perspective
Abstract
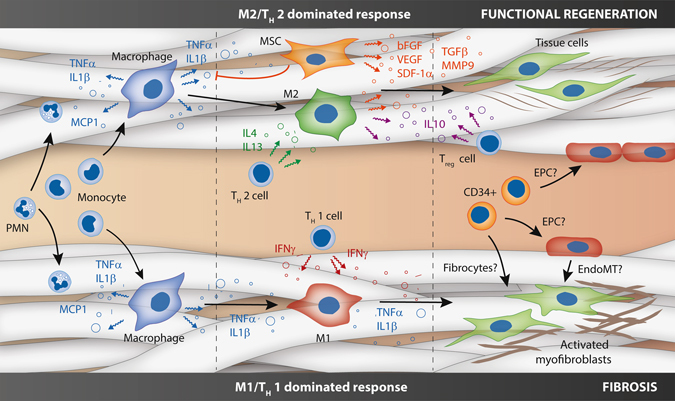
There is a persistent and growing clinical need for readily-available substitutes for heart valves and small-diameter blood vessels. In situ tissue engineering is emerging as a disruptive new technology, providing ready-to-use biodegradable, cell-free constructs which are designed to induce regeneration upon implantation, directly in the functional site. The induced regenerative process hinges around the host response to the implanted biomaterial and the interplay between immune cells, stem/progenitor cell and tissue cells in the microenvironment provided by the scaffold in the hemodynamic environment. Recapitulating the complex tissue microstructure and function of cardiovascular tissues is a highly challenging target. Therein the scaffold plays an instructive role, providing the microenvironment that attracts and harbors host cells, modulating the inflammatory response, and acting as a temporal roadmap for new tissue to be formed. Moreover, the biomechanical loads imposed by the hemodynamic environment play a pivotal role. Here, we provide a multidisciplinary view on in situ cardiovascular tissue engineering using synthetic scaffolds; starting from the state-of-the art, the principles of the biomaterial-driven host response and wound healing and the cellular players involved, toward the impact of the biomechanical, physical, and biochemical microenvironmental cues that are given by the scaffold design. To conclude, we pinpoint and further address the main current challenges for in situ cardiovascular regeneration, namely the achievement of tissue homeostasis, the development of predictive models for long-term performances of the implanted grafts, and the necessity for stratification for successful clinical translation.
Conflict of interest statement
Prof. Bouten is shareholder of Xeltis BV. Ms. Wissing, Ms. Bonito and Dr. Smits declare no potential competing financial interests.
Figures



References
-
- van Loon, S. L. M., Smits, A. I. P. M., Driessen-Mol, A., Baaijens, F. P. T. & Bouten, C. V. C. The Immune Response in In Situ Tissue Engineering of Aortic Heart Valves. Calcific Aortic Valve Disease (ed. Aikawa, E.) 207–245 (2013).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
