

Robotic and endoscopic transoral thyroidectomy: feasibility and description of the technique in the cadaveric model
- PMID: 29302476
- PMCID: PMC5750317
- DOI: 10.21037/gs.2017.10.03
Robotic and endoscopic transoral thyroidectomy: feasibility and description of the technique in the cadaveric model
Abstract
Background: Numerous new approaches have been described over the years to improve the cosmetic outcomes of thyroid surgery. Transoral approach is a new technique that aims to achieve superior cosmetic outcomes by concealing the incision in the oral cavity.
Methods: Transoral thyroidectomy through vestibular approach was performed in two institutions on cadaveric models. Procedure was performed endoscopically in one institution, while the robotic technique was utilized at the other.
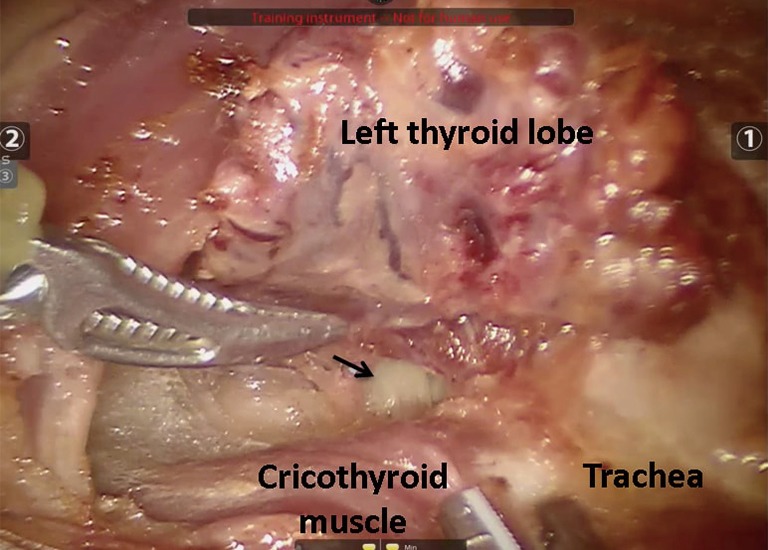
Results: Transoral thyroidectomy was successfully performed at both institutions with robotic and endoscopic techniques. All vital structures were identified and preserved.
Conclusions: Transoral thyroidectomy has been performed in animal and cadaveric models, as well as in some clinical studies. Our initial experience indicates the feasibility of this approach. More clinical studies are required to elucidate its full utility.
Keywords: Robotic; endoscopic; thyroidectomy; transoral.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures









References
LinkOut - more resources
Full Text Sources
Other Literature Sources