

Proxy and patient reports of health-related quality of life in a national cancer survey
- PMID: 29304818
- PMCID: PMC5756370
- DOI: 10.1186/s12955-017-0823-5
Proxy and patient reports of health-related quality of life in a national cancer survey
Abstract
Background: Proxy respondents are frequently used in surveys, including those assessing health-related quality of life (HRQOL). In cancer, most research involving proxies has been undertaken with paired proxy-patient populations, where proxy responses are compared to patient responses for the same individual. In these populations, proxy-patient differences are small and suggest proxy underestimation of patient HRQOL. In practice, however, proxy responses will only be used when patient responses are not available. The difference between proxy and patient reports of patient HRQOL where patients are not able to report for themselves in cancer is not known. The objective of this study was to evaluate the difference between patient and proxy reports of patient HRQOL in a large national cancer survey, and determine if this difference could be mitigated by adjusting for clinical and sociodemographic information about patients.
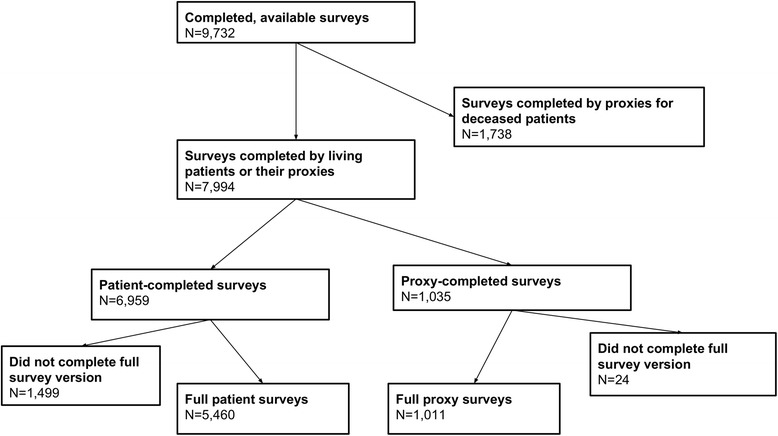
Methods: Data were from the Cancer Care Outcomes Research and Surveillance (CanCORS) study. Patients or their proxies were recruited within 3-6 months of diagnosis with lung or colorectal cancer. HRQOL was measured using the SF-12 mental and physical composite scales. Differences of ½ SD (=5 points) were considered clinically significant. The primary independent variable was proxy status. Linear regression models were used to adjust for patient sociodemographic and clinical covariates, including cancer stage, patient age and education, and patient co-morbidities.
Results: Of 6471 respondents, 1011 (16%) were proxies. Before adjustment, average proxy-reported scores were lower for both physical (-6.7 points, 95% CI -7.4 to -5.9) and mental (-6 points, 95% CI -6.7 to -5.2) health. Proxy-reported scores remained lower after adjustment (physical: -5.8 points, -6.6 to -5; mental: -5.8 points, -6.6 to 5). Proxy-patient score differences remained clinically and statistically significant, even after adjustment for sociodemographic and clinical variables.
Conclusions: Proxy-reported outcome scores for both physical and mental health were clinically and significantly lower than patient-reported scores for these outcomes. The size of the proxy-patient score differences was not affected by the health domain, and adjustment for sociodemographic and clinical variables had minimal impact.
Keywords: Cancer; Mental health; Patient-reported outcomes; Physical health; Proxy-reported outcomes; Survey.
Conflict of interest statement
Ethics approval and consent to participate
The CanCORS study was approved by institutional review boards at all participating institutions. Informed consent was obtained from all participants; at two sites, written consent was obtained and verbal consent was obtained from participants at other sites.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Similar articles
-
Differences between Proxy and Patient Assessments of Cancer Care Experiences and Quality Ratings.Health Serv Res. 2018 Apr;53(2):919-943. doi: 10.1111/1475-6773.12672. Epub 2017 Mar 2. Health Serv Res. 2018. PMID: 28255988 Free PMC article.
-
Patient and proxy reports regarding the experience of treatment decision-making in cancer care.Psychooncology. 2020 Nov;29(11):1943-1950. doi: 10.1002/pon.5528. Epub 2020 Sep 27. Psychooncology. 2020. PMID: 32840909 Free PMC article.
-
Differences in proxy-reported and patient-reported outcomes: assessing health and functional status among medicare beneficiaries.BMC Med Res Methodol. 2015 Aug 12;15:62. doi: 10.1186/s12874-015-0053-7. BMC Med Res Methodol. 2015. PMID: 26264727 Free PMC article.
-
The Association of Proxy Care Engagement with Proxy Reports of Patient Experience and Quality of Life.Health Serv Res. 2018 Oct;53(5):3809-3824. doi: 10.1111/1475-6773.12980. Epub 2018 May 27. Health Serv Res. 2018. PMID: 29806212 Free PMC article.
-
The use of proxies and proxy-reported measures: a report of the international society for quality of life research (ISOQOL) proxy task force.Qual Life Res. 2022 Feb;31(2):317-327. doi: 10.1007/s11136-021-02937-8. Epub 2021 Jul 12. Qual Life Res. 2022. PMID: 34254262 Review.
Cited by
-
Employing cognitive interviewing to evaluate, improve and validate items for measuring the health-related quality of life of women diagnosed with ovarian cancer.BMC Womens Health. 2022 Sep 27;22(1):391. doi: 10.1186/s12905-022-01966-w. BMC Womens Health. 2022. PMID: 36163023 Free PMC article.
-
Statistical considerations in long-term efficacy evaluation of anti-cancer therapies.Front Pharmacol. 2023 Oct 3;14:1265953. doi: 10.3389/fphar.2023.1265953. eCollection 2023. Front Pharmacol. 2023. PMID: 37854717 Free PMC article. Review.
-
Statistical Considerations for Embedded Pragmatic Clinical Trials in People Living with Dementia.J Am Geriatr Soc. 2020 Jul;68 Suppl 2(Suppl 2):S68-S73. doi: 10.1111/jgs.16616. J Am Geriatr Soc. 2020. PMID: 32589276 Free PMC article.
-
One year follow-up and exploratory analysis of a patient-centered interdisciplinary care intervention for multimorbidity.J Multimorb Comorb. 2021 Nov 17;11:26335565211039780. doi: 10.1177/26335565211039780. eCollection 2021 Jan-Dec. J Multimorb Comorb. 2021. PMID: 34820337 Free PMC article.
-
Factors associated with persistently high-cost health care utilization for musculoskeletal pain.PLoS One. 2019 Nov 11;14(11):e0225125. doi: 10.1371/journal.pone.0225125. eCollection 2019. PLoS One. 2019. PMID: 31710655 Free PMC article.
References
-
- Centers for Medicare and Medicaid Services: HOS and the Medicare Star Ratings [http://www.hosonline.org/en/hos-and-the-star-ratings/]. Accessed 17 Mar 2016.
-
- Strong LE. The past, present, and future of patient-reported outcomes in oncology. Am Soc Clin Oncol Educ Book. 2015:e616–20. 10.14694/EdBook_AM.2015.35.e616. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
