

Osteoporotic fractures and obesity affect frailty progression: a longitudinal analysis of the Canadian multicentre osteoporosis study
- PMID: 29304836
- PMCID: PMC5756402
- DOI: 10.1186/s12877-017-0692-0
Osteoporotic fractures and obesity affect frailty progression: a longitudinal analysis of the Canadian multicentre osteoporosis study
Abstract
Background: Despite knowing better how to screen older adults, understanding how frailty progression might be modified is unclear. We explored effects of modifiable and non-modifiable factors on changes in frailty in community-dwelling adults aged 50+ years who participated in the Canadian Multicentre Osteoporosis Study (CaMos).
Methods: Rates of change in frailty over 10 years were examined using the 30-item CaMos Frailty Index (CFI). Incident and prevalent low-trauma fractures were categorized by fracture site into hip, clinical vertebral and non-hip-non-vertebral fractures. Multivariable generalized estimating equation models accounted for the time of frailty assessment (baseline, 5 and 10 years), sex, age, body mass index (BMI, kg/m2), physical activity, bone mineral density, antiresorptive therapy, health-related quality of life (HRQL), cognitive status, and other factors for frailty or fractures. Multiple imputation and scenario analyses addressed bias due to attrition or missing data.
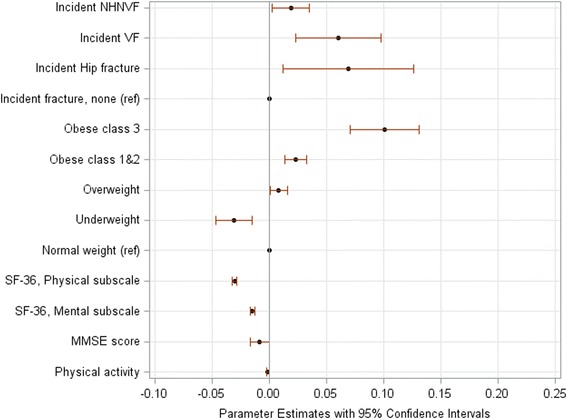
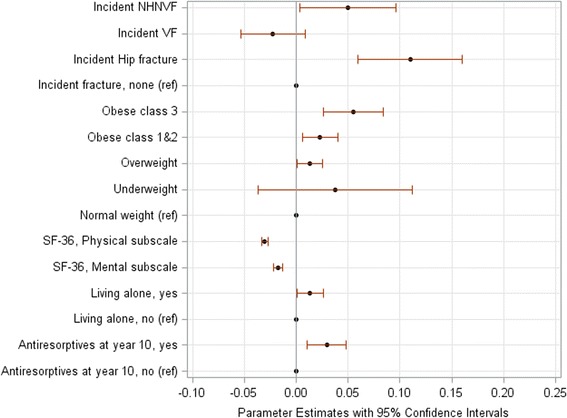
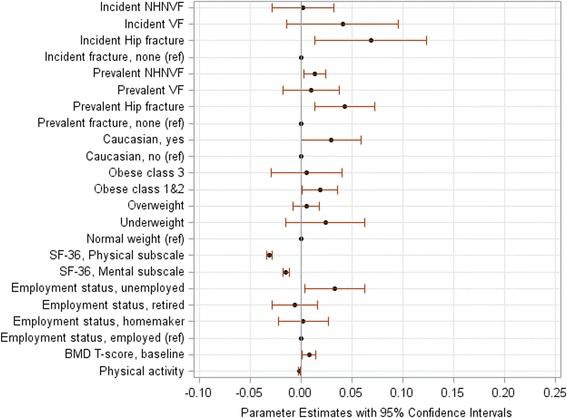
Results: The cohort included 5566 women (mean ± standard deviation: 66.8 ± 9.3 years) and 2187 men (66.3 ± 9.5 years) with the mean baseline CFI scores of 0.15 ± 0.11 and 0.12 ± 0.10, respectively. Incident fractures and obesity most strongly predicted frailty progression in multivariable analyses. The impact of fractures differed between the sexes. With each incident hip fracture, the adjusted mean CFI accelerated per 5 years by 0.07 in women (95% confidence interval [CI]: 0.03 to 0.11) and by 0.12 in men (95% CI: 0.08 to 0.16). An incident vertebral fracture increased frailty in women (0.05, 95% CI: 0.02 to 0.08) but not in men (0.01, 95% CI: -0.07 to 0.09). Irrespective of sex and prevalent fractures, baseline obesity was associated with faster frailty progression: a 5-year increase in the adjusted mean CFI ranged from 0.01 in overweight (BMI: 25.0 to 29.9 kg/m2) to 0.10 in obese individuals (BMI: ≥ 40 kg/m2). Greater physical activity and better HRQL decreased frailty over time. The results remained robust in scenario analyses.
Conclusions: Older women and men with new vertebral fractures, hip fractures or obesity represent high-risk groups that should be considered for frailty interventions.
Keywords: Changes over time; Fractures; Frailty; Longitudinal analysis; Obesity.
Conflict of interest statement
Ethics approval and consent to participate
This research was approved by the HIREB (Hamilton Integrated Research Ethics Board) a Collaboration of Hamilton Health Sciences, McMaster University, St. Joseph’s Healthcare Hamilton (RP# 94–1200). Written consent for participation in the CaMos study was obtained from all participants prior to any CaMos study activities commencing.
Review Boards that approved the CaMos study are:
McGill University Health Centres-Montreal General Hospital Research Ethics Committee.
Conjoint Health Research Ethics Board of the Faculty of Medicine, University of Calgary.
St. Joseph’s Healthcare, McMaster University Research Ethics Board.
Queen’s University Research Ethics Board.
Memorial University of Newfoundland, Human Investigations Committee.
University of Saskatchewan Advisory Committee on Ethics in Human Experimentation.
St. Michael’s Hospital Research Ethics Board (from 1996 to Winter 2017) and University Health Network Research Ethics Board (currently) (Toronto).
Capital Health Research Ethics Board (Halifax).
The University of British Columbia Clinical Research Ethics Board.
Centre hospitalier de l’Université Laval Comite d’Ethique de la Recherche Clinique.
Consent for publication
Not Applicable.
Competing interests
O. Gajic-Veljanoski (OGV), C. Kennedy (CK), G. Ioannidis (GI), C. Berger (CB), A.K.O. Wong (AW), K. Rockwood (KR), S. Kirkland (SK), P. Raina (PR) and L. Thabane (LT) declare no conflict of interests. J.D. Adachi (JDA) received grant funding, and is on advisory boards and speaker for Amgen, Eli Lilly and Merck. A. Papaioannou (AP) received grant funding and honorarium from Amgen and Eli Lilly. Kenneth Rockwood (KR) is President and Chief Scientific Officer of DGI Clinical, which has contracts with pharma on individualized outcome measurement. In July 2015 he gave a lecture at the Alzheimer Association International Conference in a symposium sponsored by Otsuka and Lundbeck. At that time, he presented at an Advisory Board meeting for Nutricia. He plans to attend a 2017 advisory board meeting for Lundbeck. Kenneth Rockwood is a member of the Research Executive Committee of the Canadian Consortium on Neurodegeneration in Aging, which is funded by the Canadian Institutes of Health Research, with additional funding from the Alzheimer Society of Canada and several other charities, as well as from Pfizer Canada and Sanofi Canada. He receives career support from the Dalhousie Medical Research Foundation as the Kathryn Allen Weldon Professor of Alzheimer Research, and research support from the Nova Scotia Health Research Foundation, the Capital Health Research Fund and the Fountain Family Innovation Fund of the Nova Scotia Health Authority Foundation.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- United Nations, Department of Economic and Social Affairs, Population Division (2015) World Population Prospects: The 2015 Revision, Key Findings and Advance Tables.Working Paper No. ESA/P/WP.241. Available from: https://esa.un.org/unpd/wpp/publications/files/key_findings_wpp_2015.pdf. Accessed 06 May 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
