

Real-world treatment of hepatitis C with second-generation direct-acting antivirals: initial results from a multicentre Canadian retrospective cohort of diverse patients
- PMID: 29305405
- PMCID: PMC5963434
- DOI: 10.9778/cmajo.20170059
Real-world treatment of hepatitis C with second-generation direct-acting antivirals: initial results from a multicentre Canadian retrospective cohort of diverse patients
Abstract
Background: High hepatitis C cure rates have been observed in registration trials with second-generation direct-acting antivirals. Real-world data also indicate high sustained viral response (SVR) rates. Our objective was to determine real-world SVR rates for patients infected with hepatitis C virus (HCV) who were treated with second-generation direct-acting antivirals in the first 18 months of their availability in Canada.
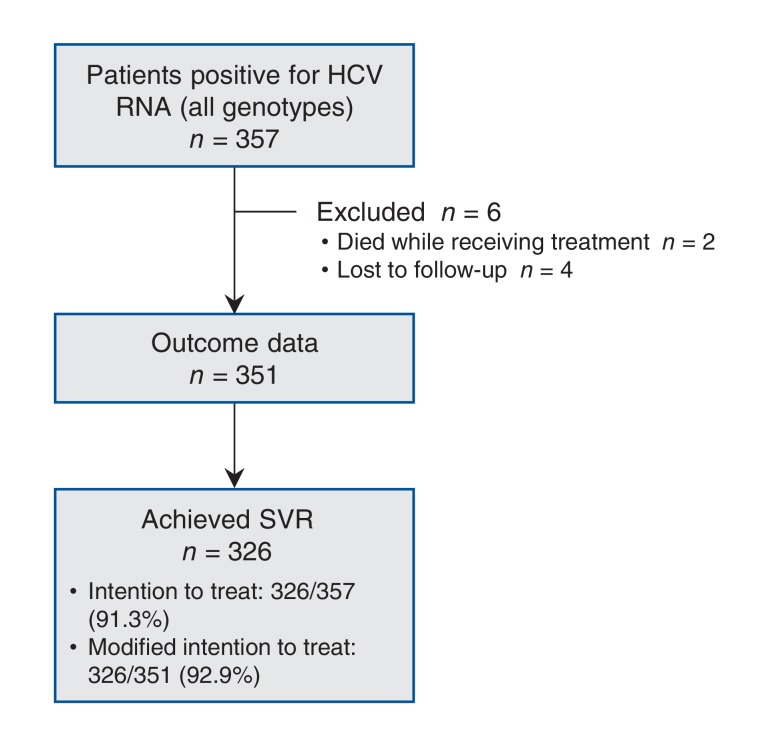
Methods: Four centres in Calgary contributed their treatment data for a diverse patient population including those who had or had not undergone liver transplantation, those coinfected with HIV and vulnerable populations. We included all patients documented to have started hepatitis C treatment with direct-acting antivirals between October 2014 and April 2016, with follow-up through October 2016. We used multivariate analysis to determine independent predictors of treatment failure.
Results: Outcome data were available for 351 patients, of whom 326 (92.9%) achieved an SVR (193/206 [93.7%], 57/59 [96.6%] and 44/51 [86.3%] for genotypes 1a, 1b and 3, respectively, p = 0.2). Independent predictors of not achieving SVR were older age (adjusted odds ratio [OR] 0.95 [95% confidence interval (CI) 0.90-1.00]), male sex (adjusted OR 0.30 [95% CI 0.10-0.89]) and, in patients with genotype 1a infection, history of hepatocellular carcinoma (adjusted OR 0.13 [95% CI 0.03-0.53]). In the entire cohort, the presence of cirrhosis, genotype and hepatocellular carcinoma were not associated with a lower SVR rate. There were no differences in SVR rate according to treatment centre, HIV coinfection or liver transplantation. Among patients with genotype 3 infection, a significantly lower SVR rate was observed for those treated outside of standard of care than for those treated within standard of care (33.3% v. 89.6%, p = 0.04). De novo hepatocellular carcinoma developed in 12 patients (3.4%) despite successful direct-acting antiviral therapy.
Interpretation: We report high SVR rates in a real-world diverse cohort of HCV-infected patients treated with second-generation direct-acting antivirals. The results highlight the importance of conducting real-world analyses to elucidate clinical factors associated with poorer outcomes that may not be identified in registration trials.
Copyright 2018, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: See the end of the article.
Figures
References
-
- Afdhal N, Zeuzem S, Kwo P, et al. ION-1 Investigators. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med. 2014;370:1889–98. - PubMed
-
- Kowdley KV, Gordon SC, Reddy KR, et al. ION-3 Investigators. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370:1879–88. - PubMed
-
- Afdhal N, Reddy KR, Nelson DR, et al. ION-2 Investigators. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N Engl J Med. 2014;370:1483–93. - PubMed
-
- Ferenci P, Bernstein D, Lalezari J, et al. PEARL-III StudyPEARL-IV Study. ABT-450/r-ombitasvir and dasabuvir with or without ribavirin for HCV. N Engl J Med. 2014;370:1983–92. - PubMed
-
- Hézode C, Fontaine H, Dorival C, et al. CUPIC Study Group. Effectiveness of telaprevir or boceprevir in treatment-experienced patients with HCV genotype 1 infection and cirrhosis. Gastroenterology. 2014;147:132–42.e4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous