

False-Positive Xpert MTB/RIF Results in Retested Patients with Previous Tuberculosis: Frequency, Profile, and Prospective Clinical Outcomes
- PMID: 29305538
- PMCID: PMC5824043
- DOI: 10.1128/JCM.01696-17
False-Positive Xpert MTB/RIF Results in Retested Patients with Previous Tuberculosis: Frequency, Profile, and Prospective Clinical Outcomes
Abstract
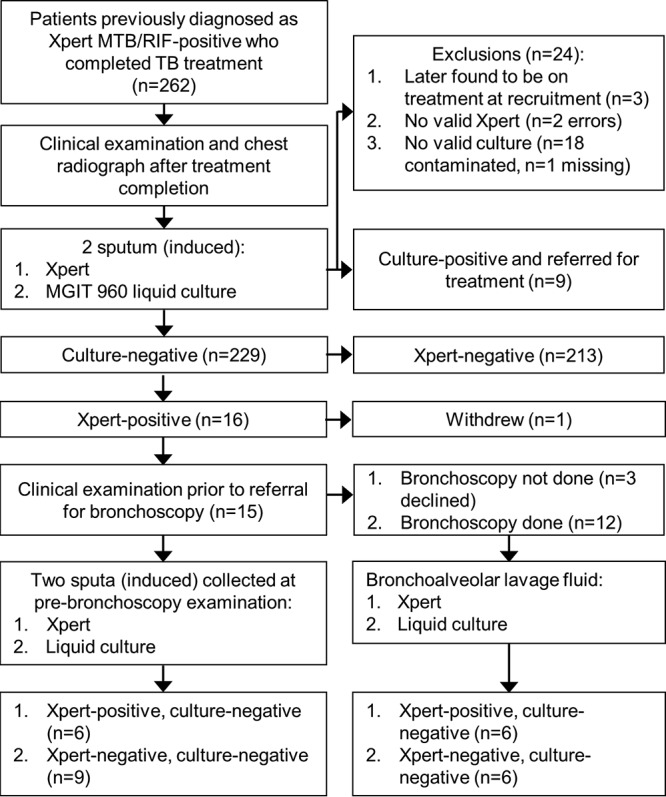
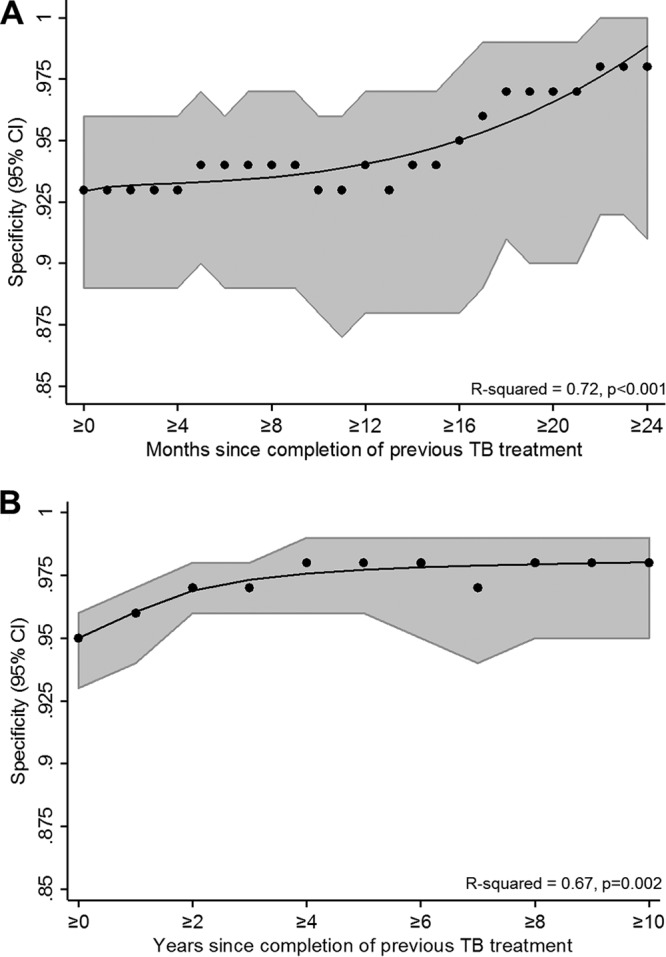
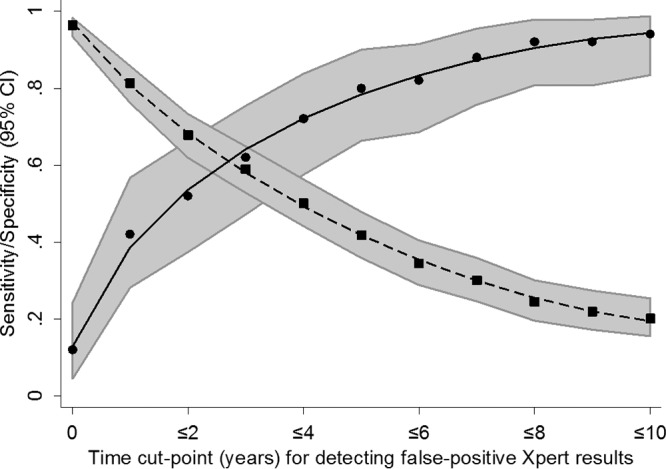
Globally, Xpert MTB/RIF (Xpert) is the most widely used PCR test for the diagnosis of tuberculosis (TB). Positive results in previously treated patients, which are due to old DNA or active disease, are a diagnostic dilemma. We prospectively retested sputum from 238 patients, irrespective of current symptoms, who were previously diagnosed to be Xpert positive and treated successfully. Patients who retested as Xpert positive and culture negative were exhaustively investigated (repeat culture, chest radiography, bronchoscopy with bronchoalveolar lavage, long-term clinical follow-up). We evaluated whether the duration since previous treatment completion, mycobacterial burden (the Xpert cycle threshold [CT ] value), and reclassification of Xpert-positive results with a very low semiquantitation level to Xpert-negative results reduced the rate of false positivity. A total of 229/238 (96%) of patients were culture negative. Sixteen of 229 (7%) were Xpert positive a median of 11 months (interquartile range, 5 to 19 months) after treatment completion. The specificity was 93% (95% confidence interval [CI], 89 to 96%). Nine of 15 (40%) Xpert-positive, culture-negative patients reverted to Xpert negative after 2 to 3 months (1 patient declined further participation). Patients with false-positive Xpert results had a lower mycobacterial burden than patients with true-positive Xpert results (CT , 28.7 [95% CI, 27.2 to 30.4] versus 17.6 [95% CI, 16.9 to 18.2]; P < 0.001), an increased likelihood of a chest radiograph not compatible with active TB (5/15 patients versus 0/5 patients; P = 0.026), and less-viscous sputum (15/16 patients versus 2/5 patients whose sputum was graded as mucoid or less; P = 0.038). All patients who initially retested as Xpert positive and culture negative ("Xpert false positive") were clinically well without treatment after follow-up. The duration since the previous treatment poorly predicted false-positive results (a duration of ≤2 years identified only 66% of patients with false-positive results). Reclassifying Xpert-positive results with a very low semiquantitation level to Xpert negative improved the specificity (+3% [95% CI, +2 to +5%]) but reduced the sensitivity (-10% [95% CI, -4 to -15%]). Patients with previous TB retested with Xpert can have false-positive results and thus not require treatment. These data inform clinical practice by highlighting the challenges in interpreting Xpert-positive results, underscore the need for culture, and have implications for next-generation ultrasensitive tests.
Keywords: Mycobacterium tuberculosis.
Copyright © 2018 American Society for Microbiology.
Figures
References
-
- Monkongdee P, McCarthy KD, Cain KP, Tasaneeyapan T, Dung NH, Lan NTN, Yen NTB, Teeratakulpisarn N, Udomsantisuk N, Heilig C. 2009. Yield of acid-fast smear and mycobacterial culture for tuberculosis diagnosis in people with human immunodeficiency virus. Am J Respir Crit Care Med 180:903. doi: 10.1164/rccm.200905-0692OC. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
