

Multicenter Evaluation of the Accelerate PhenoTest BC Kit for Rapid Identification and Phenotypic Antimicrobial Susceptibility Testing Using Morphokinetic Cellular Analysis
- PMID: 29305546
- PMCID: PMC5869823
- DOI: 10.1128/JCM.01329-17
Multicenter Evaluation of the Accelerate PhenoTest BC Kit for Rapid Identification and Phenotypic Antimicrobial Susceptibility Testing Using Morphokinetic Cellular Analysis
Abstract
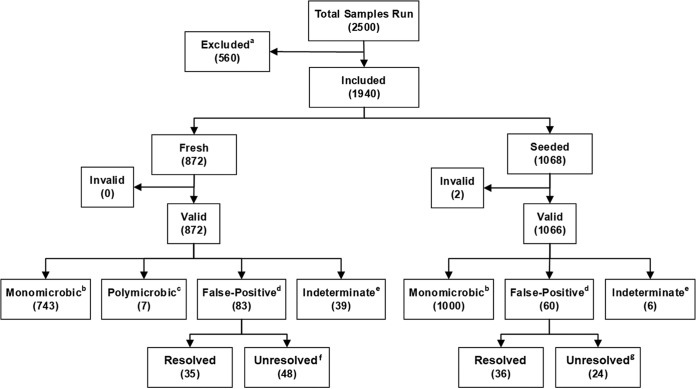
We describe results from a multicenter study evaluating the Accelerate Pheno system, a first of its kind diagnostic system that rapidly identifies common bloodstream pathogens from positive blood cultures within 90 min and determines bacterial phenotypic antimicrobial susceptibility testing (AST) results within ∼7 h. A combination of fresh clinical and seeded blood cultures were tested, and results from the Accelerate Pheno system were compared to Vitek 2 results for identification (ID) and broth microdilution or disk diffusion for AST. The Accelerate Pheno system accurately identified 14 common bacterial pathogens and two Candida spp. with sensitivities ranging from 94.6 to 100%. Of fresh positive blood cultures, 89% received a monomicrobial call with a positive predictive value of 97.3%. Six common Gram-positive cocci were evaluated for ID. Five were tested against eight antibiotics, two resistance phenotypes (methicillin-resistant Staphylococcus aureus and Staphylococcus spp. [MRSA/MRS]), and inducible clindamycin resistance (MLSb). From the 4,142 AST results, the overall essential agreement (EA) and categorical agreement (CA) were 97.6% and 97.9%, respectively. Overall very major error (VME), major error (ME), and minor error (mE) rates were 1.0%, 0.7%, and 1.3%, respectively. Eight species of Gram-negative rods were evaluated against 15 antibiotics. From the 6,331 AST results, overall EA and CA were 95.4% and 94.3%, respectively. Overall VME, ME, and mE rates were 0.5%, 0.9%, and 4.8%, respectively. The Accelerate Pheno system has the unique ability to identify and provide phenotypic MIC and categorical AST results in a few hours directly from positive blood culture bottles and support accurate antimicrobial adjustment.
Keywords: FISH; MIC; antimicrobial susceptibility testing; bacteremia; blood culture; candidemia; identification; morphokinetic cellular analysis; phenotypic; rapid.
Copyright © 2018 Pancholi et al.
Figures
Comment in
-
The Slow March toward Rapid Phenotypic Antimicrobial Susceptibility Testing: Are We There Yet?J Clin Microbiol. 2018 Mar 26;56(4):e01999-17. doi: 10.1128/JCM.01999-17. Print 2018 Apr. J Clin Microbiol. 2018. PMID: 29436417 Free PMC article.
References
-
- Sutton JP, Friedman B. 2006. Trends in septicemia hospitalizations and readmissions in selected HCUP states, 2005 and 2010. Statistical Brief #161. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Agency for Healthcare Research and Quality, US Department of Health and Human Services, Rockville, MD. - PubMed
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M. 2006. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34:1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
-
- Buehler SS, Madison B, Snyder SR, Derzon JH, Cornish NE, Saubolle MA, Weissfeld AS, Weinstein MP, Liebow EB, Wolk DM. 2016. Effectiveness of practices to increase timeliness of providing targeted therapy for inpatients with bloodstream infections: a laboratory medicine best practices systematic review and meta-analysis. Clin Microbiol Rev 29:59–103. doi: 10.1128/CMR.00053-14. - DOI - PMC - PubMed
-
- Retamar P, Portillo MM, Lopez-Prieto MD, Rodriguez-Lopez F, de Cueto M, Garcia MV, Gomez MJ, Del Arco A, Munoz A, Sanchez-Porto A, Torres-Tortosa M, Martin-Aspas A, Arroyo A, Garcia-Figueras C, Acosta F, Corzo JE, Leon-Ruiz L, Escobar-Lara T, Rodriguez-Bano J, SAEI/SAMPAC Bacteremia Group. 2012. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis. Antimicrob Agents Chemother 56:472–478. doi: 10.1128/AAC.00462-11. - DOI - PMC - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, et al. 2017. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med 45:486–552. doi: 10.1097/CCM.0000000000002255. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
