

Trends in cardiovascular risk factor and disease prevalence in patients undergoing non-cardiac surgery
- PMID: 29305561
- PMCID: PMC6102124
- DOI: 10.1136/heartjnl-2017-312391
Trends in cardiovascular risk factor and disease prevalence in patients undergoing non-cardiac surgery
Abstract
Objectives: Cardiovascular risk factors are prevalent in the population undergoing non-cardiac surgery. Changes in perioperative cardiovascular risk factor profiles over time are unknown. The objective of this study was to evaluate national trends in cardiovascular risk factors and atherosclerotic cardiovascular disease (ASCVD) among patients undergoing non-cardiac surgery.
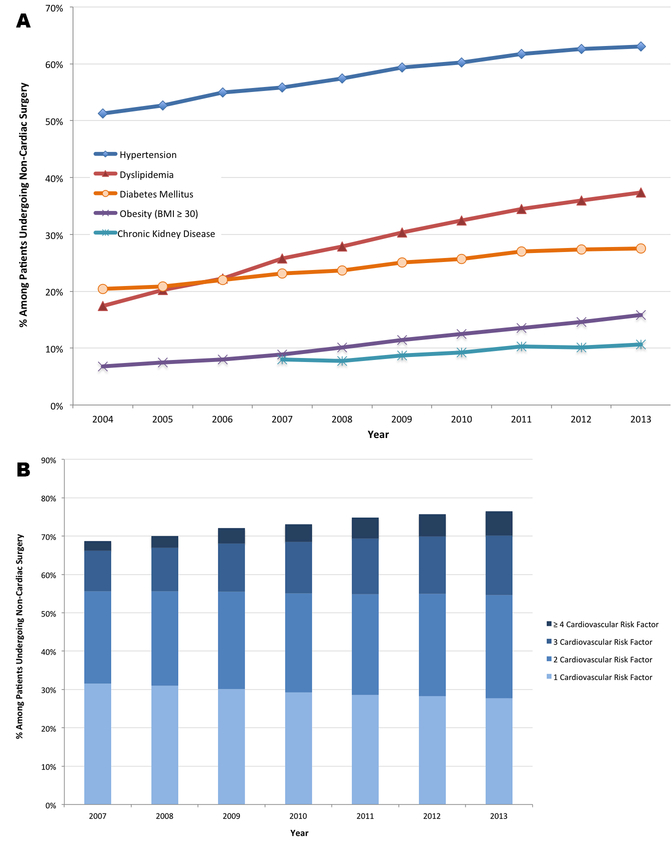
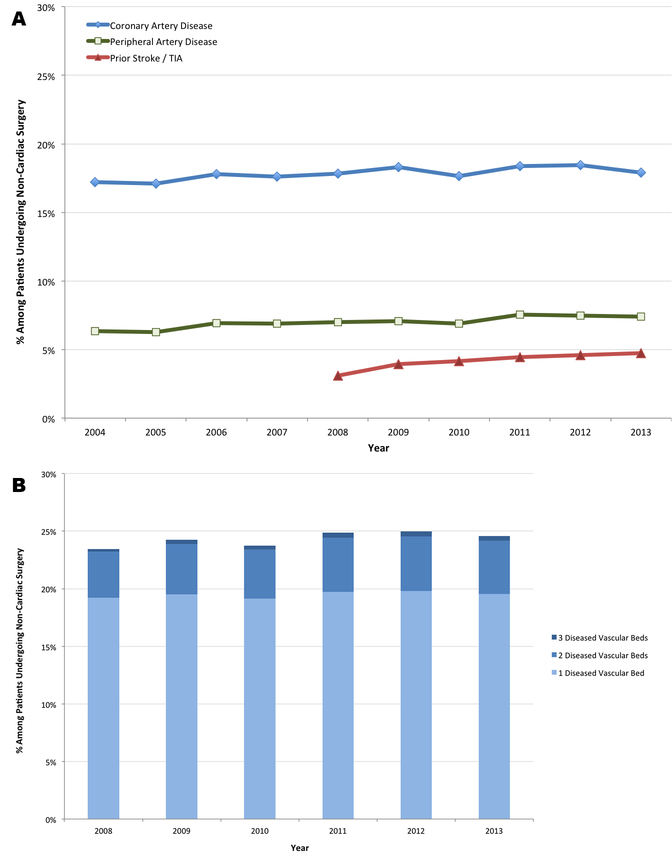
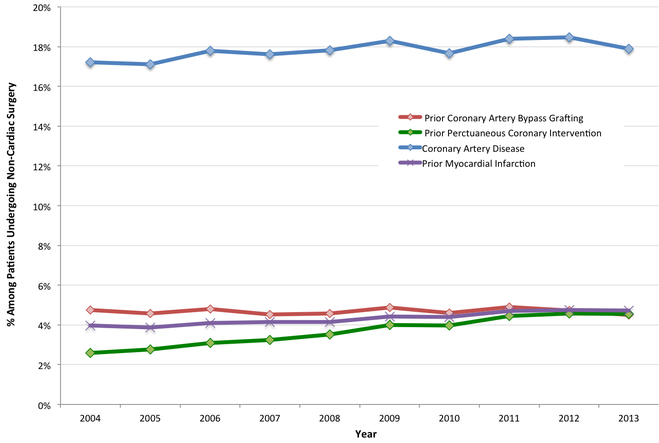
Methods: Adults aged ≥45 years old who underwent non-cardiac surgery were identified using the US National Inpatient Sample from 2004 to 2013. The prevalence of traditional cardiovascular risk factors (hypertension, dyslipidaemia, diabetes mellitus, obesity and chronic kidney disease) and ASCVD (coronary artery disease, peripheral artery disease and prior stroke] were evaluated over time.
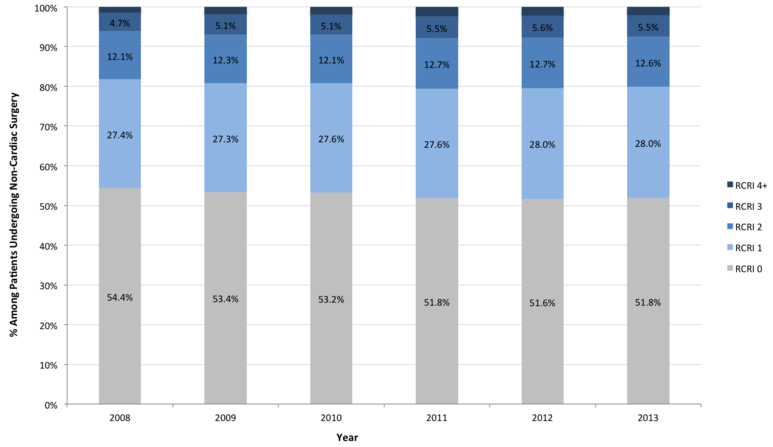
Results: A total of 10 581 621 hospitalisations for major non-cardiac surgery were identified. Between 2008 and 2013, ≥2 cardiovascular risk factors and ASCVD were present in 44.5% and 24.3% of cases, respectively. Over time, the prevalence of multiple (≥2) cardiovascular risk factors increased from 40.5% in 2008-2009 to 48.2% in 2012-2013, P<0.001. The proportion of patients with coronary artery disease (17.2% in 2004-2005 vs 18.2% in 2012-2013, P<0.001), peripheral artery disease (6.3% in 2004-2005 vs 7.4% in 2012-2013, P<0.001) and prior stroke (3.5% in 2008-2009 vs 4.7% 2012-2013, P<0.001) also increased over time. The proportion of patients with a modified Revised Cardiac Risk Index score ≥3 increased from 6.6% in 2008-2009 to 7.7% in 2012-2013 (P<0.001).
Conclusions: Among patients undergoing major non-cardiac surgery, the burden of cardiovascular risk factors and the prevalence of ASCVD increased over time. Adverse trends in risk profiles require continued attention to improve perioperative cardiovascular outcomes.
Keywords: coronary artery disease; risks factors.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JAB reports serving on advisory boards for AstraZeneca, Sanofi, Aralez and Abbott Vascular and has received research grants from Merck. The remainder of the authors report no relationships that could be construed as a conflict of interest.
Figures
References
-
- Weiser TG, Haynes AB, Molina G et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet 2015;385 Suppl 2:S11. - PubMed
-
- Goldman L, Caldera DL, Nussbaum SR et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med 1977;297:845–50. - PubMed
-
- Lee TH, Marcantonio ER, Mangione CM et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100:1043–9. - PubMed
-
- Gupta PK, Gupta H, Sundaram A et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation 2011;124:381–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical