

Disease Course and Treatment Responses in Children With Relapsing Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease
- PMID: 29305608
- PMCID: PMC5885190
- DOI: 10.1001/jamaneurol.2017.4601
Disease Course and Treatment Responses in Children With Relapsing Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease
Abstract
Importance: Myelin oligodendrocyte glycoprotein antibodies (MOG-Abs) are consistently identified in a range of demyelinating disorders in adults and children. Current therapeutic strategies are largely center specific, and no treatments have been formally evaluated.
Objective: To examine the clinical phenotypes, treatment responses, and outcomes of children with relapsing MOG-Ab-associated disease.
Design, setting, and participants: This study prospectively collected demographic, clinical, and radiologic data from 102 patients from 8 countries of the EU Paediatric Demyelinating Disease Consortium from January 1, 2014, through December 31, 2016. Patients were treated according to local protocols.
Main outcomes and measures: Annualized relapse rates (ARRs) and Expanded Disability Status Scale (EDSS) scores before and during treatment with disease-modifying drugs (DMDs).
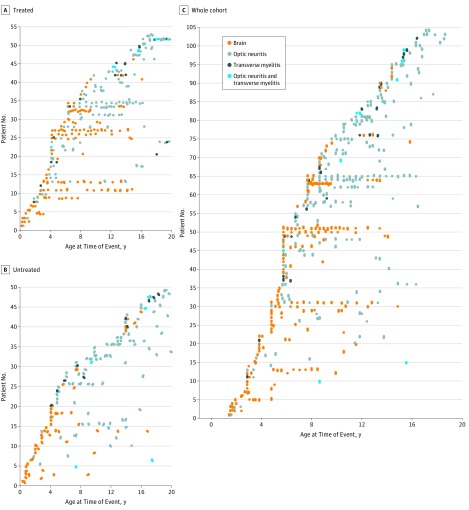
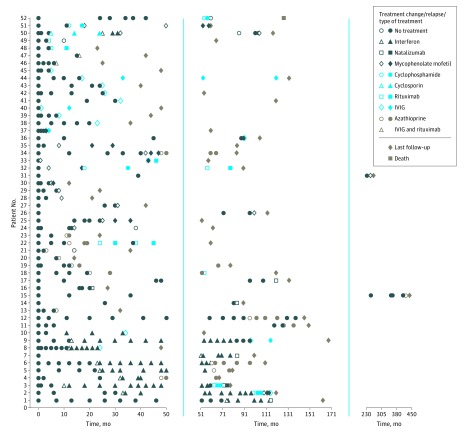
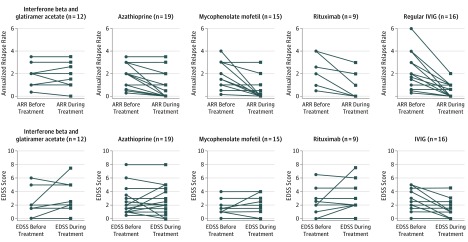
Results: A total of 102 children were identified (median [range] age, 7.0 [1.5-7.9] years; male to female ratio, 1.0:1.8; white to other race/ethnicity ratio, 3.6:1.0). Original diagnoses were neuromyelitis optica spectrum disorder (44 patients [43.1%]), acute disseminated encephalomyelitis followed by optic neuritis (20 [19.6%]), multiphasic disseminated encephalomyelitis (20 [19.6%]), and relapsing optic neuritis (18 [17.6%]). In all, 464 demyelinating events were reported. Treated patients had more relapses (median, 3.0; range, 1.0-17.0) than untreated patients (median, 1.0; range 1.0-7.0) (P = .009) and higher EDSS scores (median, 1.5; interquartile range, 0-2.5) than untreated patients (median, 1.0; interquartile range, 0-1.5) (P < .001). Fifty-two children (51.0%) received DMDs: 28 (53.8%) were treated with 1 DMD, 17 (32.7%) with 2, and 7 (13.5%) with 3 or more sequential DMDs. Patients relapsed during all treatments, with a total of 127 relapses on treatment reported. No changes in median ARR and EDSS score were observed between the preinitiation and postinitiation phases of interferon beta and glatiramer acetate treatment (n = 11). The median ARR was reduced from 1.84 to 1.0 with azathioprine (n = 20, P < .001), 1.79 to 0.52 with mycophenolate mofetil (n = 15, P = .003), and 2.12 to 0.67 with rituximab (n = 9, P < .001), although the median EDSS score remained unchanged. An improvement in ARR (from 2.16 to 0.51, P < .001) and EDSS score (from 2.2 to 1.2, P = .01) was observed in the 12 patients treated with regular intravenous immunoglobulins.
Conclusions and relevance: Although commonly used to treat patients with multiple sclerosis, DMDs were not associated with clinical improvement in children with MOG-Ab-associated disease, whereas azathioprine, mycophenolate mofetil, rituximab, and particularly intravenous immunoglobulins were associated with a reduction in relapse frequency. A correct diagnosis of relapsing MOG-Ab-associated disorders is therefore important to optimize immune treatment.
Conflict of interest statement
Figures
Comment in
-
Myelin oligodendrocyte glycoprotein antibody-associated disease: characterising clinical disease.J Neurol. 2018 Aug;265(8):1950-1952. doi: 10.1007/s00415-018-8963-z. J Neurol. 2018. PMID: 29992350 Free PMC article. No abstract available.
References
-
- Reindl M, Jarius S, Rostasy K, Berger T. Myelin oligodendrocyte glycoprotein antibodies: how clinically useful are they? Curr Opin Neurol. 2017;30(3):295-301. - PubMed
-
- Tenembaum S, Chitnis T, Nakashima I, et al. Neuromyelitis optica spectrum disorders in children and adolescents. Neurology. 2016;87(9)(suppl 2):S59-S66. - PubMed
-
- Ketelslegers IA, Van Pelt DE, Bryde S, et al. Anti-MOG antibodies plead against MS diagnosis in an acquired demyelinating syndromes cohort. Mult Scler. 2015;21(12):1513-1520. - PubMed
-
- Hennes EM, Baumann M, Schanda K, et al. ; BIOMARKER Study Group . Prognostic relevance of MOG antibodies in children with an acquired demyelinating syndrome. Neurology. 2017;89(9):900-908. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
