

Unmeasured Confounders in Observational Studies Comparing Bilateral Versus Single Internal Thoracic Artery for Coronary Artery Bypass Grafting: A Meta-Analysis
- PMID: 29306899
- PMCID: PMC5778975
- DOI: 10.1161/JAHA.117.008010
Unmeasured Confounders in Observational Studies Comparing Bilateral Versus Single Internal Thoracic Artery for Coronary Artery Bypass Grafting: A Meta-Analysis
Abstract
Background: Observational studies suggest a survival advantage with bilateral single internal thoracic artery (BITA) versus single internal thoracic artery grafting for coronary surgery, whereas this conclusion is not supported by randomized trials. We hypothesized that this inconsistency is attributed to unmeasured confounders intrinsic to observational studies. To test our hypothesis, we performed a meta-analysis of the observational literature comparing BITA and single internal thoracic artery, deriving incident rate ratio for mortality at end of follow-up and at 1 year. We postulated that BITA would not affect 1-year survival based on the natural history of coronary artery bypass occlusion, so that a difference between groups at 1 year could not be attributed to the intervention.
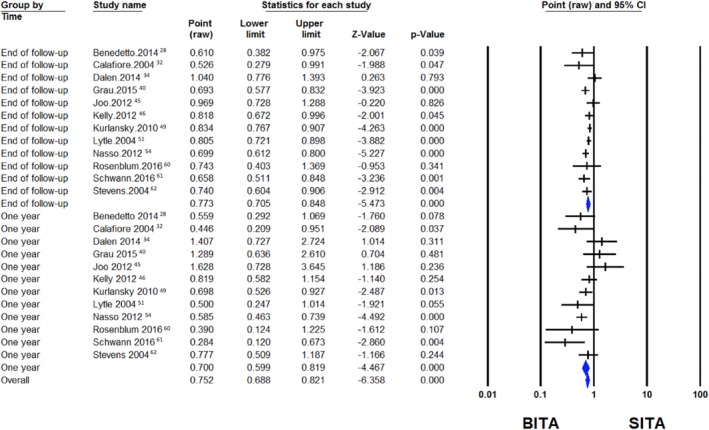
Methods and results: We searched MEDLINE and Pubmed to identify all observational studies comparing the outcome of BITA versus single internal thoracic artery. One-year and long-term mortality for BITA and single internal thoracic artery were compared in the propensity-score-matched (PSM) series, that is, the form of observational evidence less prone to confounders. Thirty-eight observational studies (174 205 total patients) were selected for final comparison. In the 12 propensity-score-matched series (34 019 patients), the mortality reduction for BITA was similar at 1 year and at the end of follow-up (incident rate ratio, 0.70; 95% confidence interval, 0.60-0.82 versus 0.77; 95% confidence interval, 0.70-0.85; P for subgroup difference=0.43).
Conclusions: Unmeasured confounders, rather than biological superiority, may explain the survival advantage of BITA in observational series.
Keywords: bypass graft; myocardial revascularization; surgery.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

Comment in
-
Right for the Wrong Reasons: Implications of Data Insufficiency in Bilateral Versus Single Internal Thoracic Artery Grafting Analysis.J Am Heart Assoc. 2018 Jan 6;7(1):e008262. doi: 10.1161/JAHA.117.008262. J Am Heart Assoc. 2018. PMID: 29306900 Free PMC article. No abstract available.
References
-
- Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW, Golding LA, Gill CC, Taylor PC, Sheldon WC. Influence of the internal‐mammary‐artery graft on 10‐year survival and other cardiac events. N Engl J Med. 1986;314:1–6. - PubMed
-
- Lytle BW, Blackstone EH, Loop FD, Houghtaling PL, Arnold JH, Akhrass R, McCarthy PM, Cosgrove DM. Two internal thoracic artery grafts are better than one. J Thorac Cardiovasc Surg. 1999;117:855–872. - PubMed
-
- Tatoulis J, Buxton BF, Fuller JA. Patencies of 2127 arterial to coronary conduits over 15 years. Ann Thorac Surg. 2004;77:93–101. - PubMed
-
- Rizzoli G, Schiavon L, Bellini P. Does the use of bilateral internal mammary artery (IMA) grafts provide incremental benefit relative to the use of a single IMA graft? A meta‐analysis approach. Eur J Cardiothorac Surg. 2002;22:781–786. - PubMed
-
- Taggart DP, D'Amico R, Altman DG. Effect of arterial revascularisation on survival: a systematic review of studies comparing bilateral and single internal mammary arteries. Lancet. 2001;358:870–875. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
