

Assessment of peri-polyp biopsy specimens of flat mucosa in patients with inflammatory bowel disease
- PMID: 29307473
- PMCID: PMC9646239
- DOI: 10.1016/j.gie.2017.12.016
Assessment of peri-polyp biopsy specimens of flat mucosa in patients with inflammatory bowel disease
Abstract
Background and aims: When colon polyps are removed in the setting of inflammatory bowel disease (IBD) involving the large intestine, biopsy sampling of the flat mucosa surrounding such polyps have been recommended, but there are no data to support this practice.
Methods: We reviewed endoscopic and pathologic findings in IBD patients who had dysplastic polyps removed and biopsy sampling of the adjacent flat mucosa. We assessed risk for subsequent neoplasia based on the presence or absence of dysplasia in the peri-polyp flat mucosa and based on number and grade of index polypoid lesions. Kaplan-Meier survival analysis was performed.
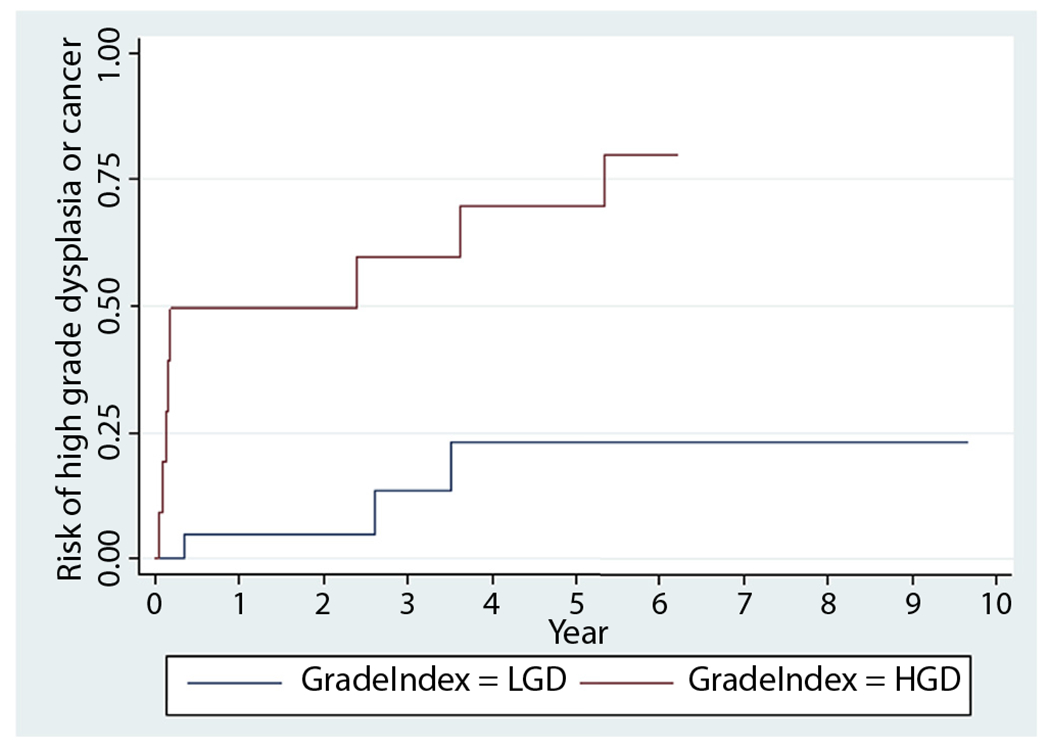
Results: Fifty-six IBD patients (68% ulcerative colitis [UC]) underwent 102 colonoscopies, in which 129 dysplastic polyps were resected. Five hundred three biopsy procedures of the surrounding flat mucosa were performed (mean, 3.9 biopsy samples per polyp), of which 16 (3.2%) were dysplastic. Thirty-four patients (21 UC) had follow-up in a median of 1.7 years (range, .02-15) and 147 colonoscopies. The presence of dysplasia in peri-polyp biopsy specimens during index colonoscopy was not associated with risk of developing high-grade dysplasia (HGD) or cancer (Pearson χ2 test = .19). The size and number of dysplastic polyps were not predictive of neoplastic outcomes, but the probability of developing subsequent advanced neoplasia for polypoid low-grade dysplasia was 18%, 29%, and 40% by 1, 3, and 5 years, respectively, and for polypoid HGD was 50%, 60%, and 70% by 1, 3, and 5 years, respectively (hazard ratio, 7.0; standard error, 4.8).
Conclusions: In patients with IBD-associated colitis, biopsy sampling of the mucosa adjacent to discrete dysplastic polypoid lesions are low yield and do not predict findings in follow-up examinations. However, the grade of dysplasia of the polyp itself is predictive of subsequent advanced neoplasia.
Copyright © 2018 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Polyp-adjacent biopsies no longer required in inflammatory bowel disease.Gastrointest Endosc. 2018 Oct;88(4):782-783. doi: 10.1016/j.gie.2018.05.005. Gastrointest Endosc. 2018. PMID: 30217249 No abstract available.
-
Response.Gastrointest Endosc. 2018 Oct;88(4):783-784. doi: 10.1016/j.gie.2018.06.014. Gastrointest Endosc. 2018. PMID: 30217250 No abstract available.
References
-
- Beaugerie L, Itzkowitz SH. Cancers complicating inflammatory bowel disease. N Engl J Med 2015;372:1441–52. - PubMed
-
- Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 2010;105:501–23; quiz 524. - PubMed
-
- Itzkowitz SH, Present DH. Consensus conference: colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis 2005;11:314–21. - PubMed
-
- Cairns SR, Scholefield JH, Steele RJ, et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002). Gut 2010;59:666–89. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
