

Editor's Choice - The Implications of Non-compliance to Endovascular Aneurysm Repair Surveillance: A Systematic Review and Meta-analysis
- PMID: 29307756
- PMCID: PMC6481561
- DOI: 10.1016/j.ejvs.2017.11.030
Editor's Choice - The Implications of Non-compliance to Endovascular Aneurysm Repair Surveillance: A Systematic Review and Meta-analysis
Abstract
Objective/background: Increasingly, reports show that compliance rates with endovascular aneurysm repair (EVAR) surveillance are often suboptimal. The aim of this study was to determine the safety implications of non-compliance with surveillance.
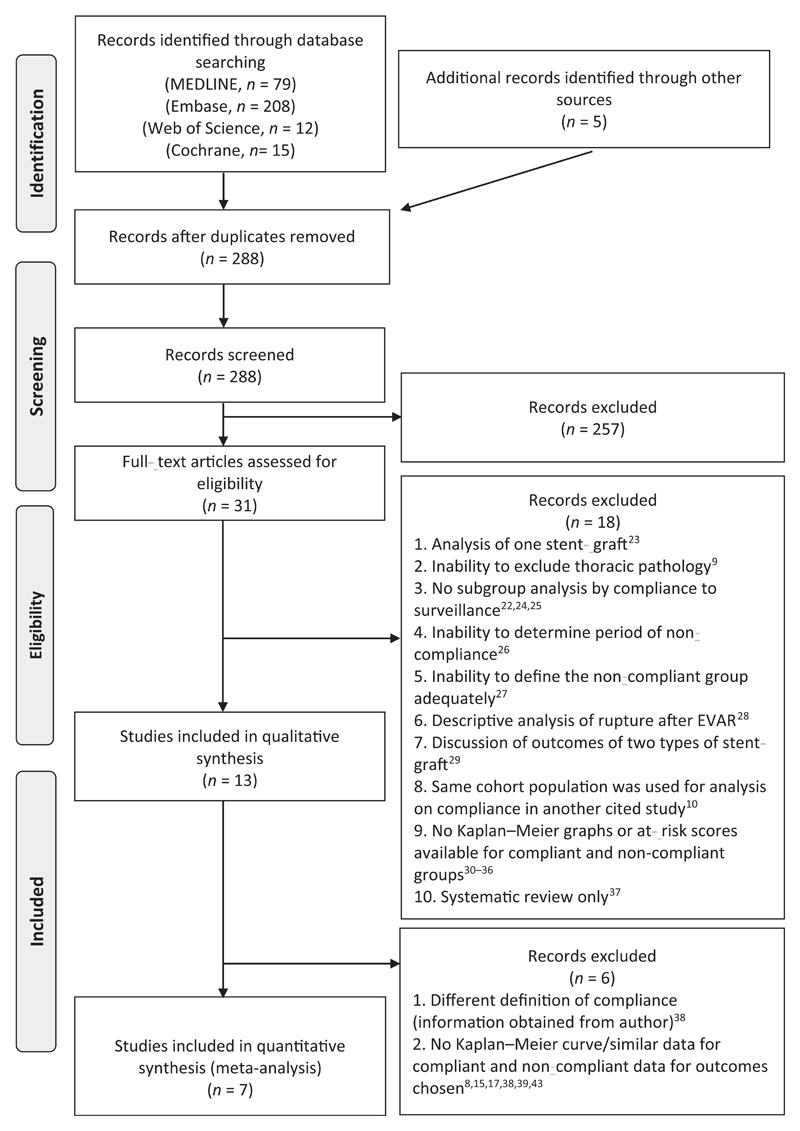
Methods: The study was carried out according to the Preferred Items for Reporting of Systematic Reviews and Meta-Analyses (PRISMA) guidelines. An electronic search was undertaken by two independent authors using Embase, MEDLINE, Cochrane, and Web of Science databases from 1990 to July 2017. Only studies that analysed infrarenal EVAR and had a definition of non-compliance described as weeks or months without imaging surveillance were analysed. Meta-analysis was carried out using the random-effects model and restricted maximum likelihood estimation.
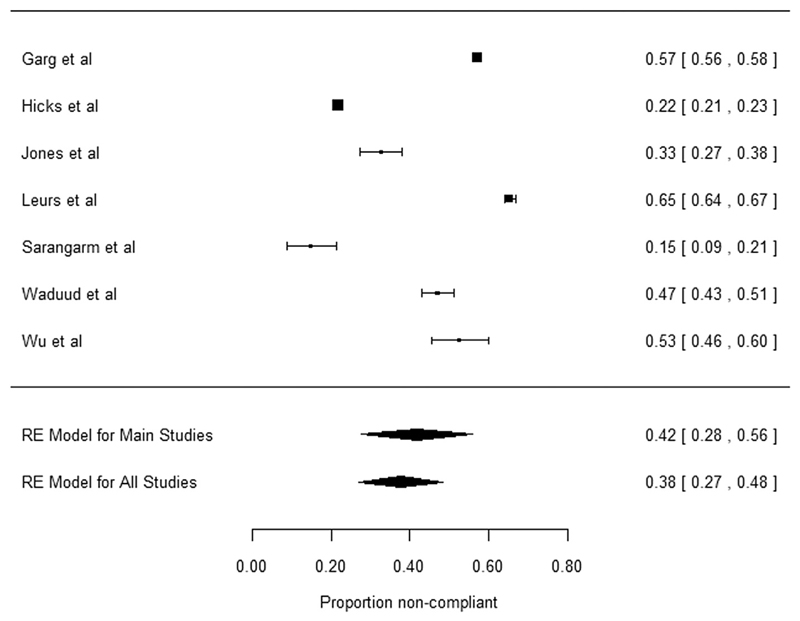
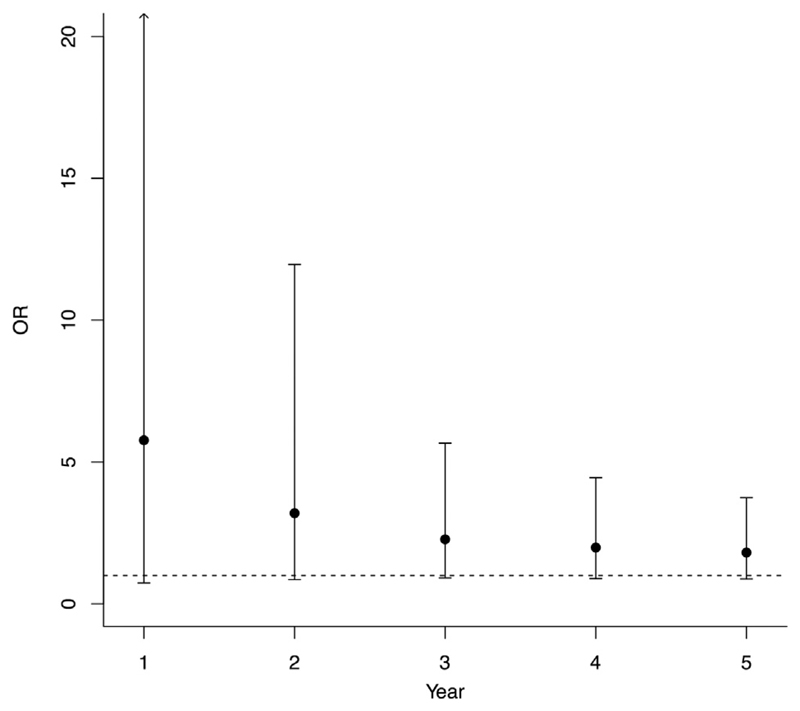
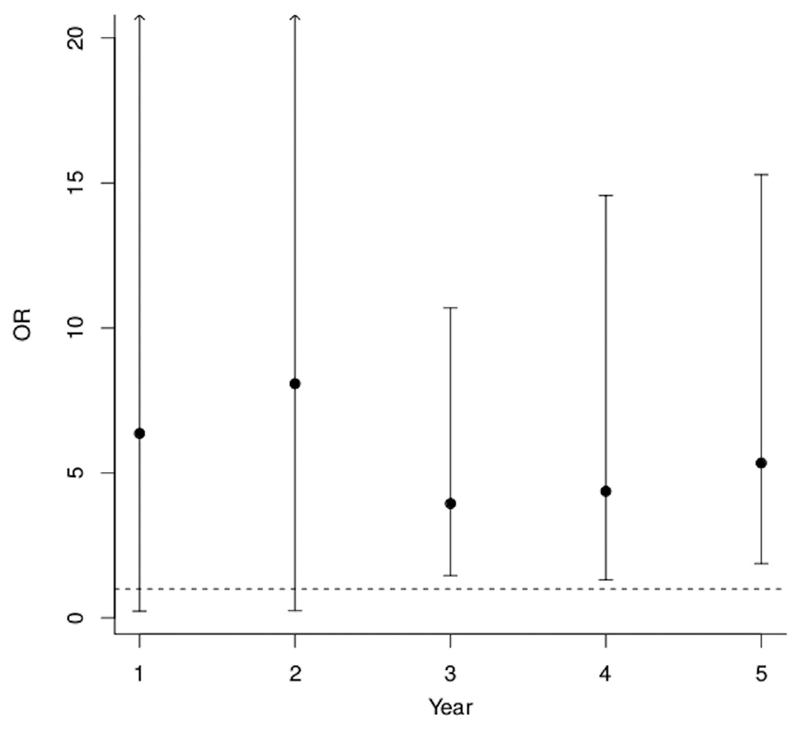
Results: Thirteen articles (40,730 patients) were eligible for systematic review; of these, seven studies (14,311 patients) were appropriate for comparative meta-analyses of mortality rates. Three studies (8316 patients) were eligible for the comparative meta-analyses of re-intervention rates after EVAR and four studies (12,995 patients) eligible for meta-analysis for abdominal aortic aneurysm related mortality (ARM). The estimated average non-compliance rate was 42.0% (95% confidence interval [CI] 28-56%). Although there is some evidence that non-compliant patients have better survival rates, there was no statistically significant difference in all cause mortality rates (year 1: odds ratio [OR] 5.77, 95% CI 0.74-45.14; year 3: OR 2.28, 95% CI 0.92-5.66; year 5: OR 1.81, 95% CI 0.88-3.74) and ARM (OR 1.47, 95% CI 0.99-2.19) between compliant and non-compliant patients in the first 5 years after EVAR. The re-intervention rate was statistically significantly higher in compliant patients from 3 to 5 years after EVAR (year 1: OR 6.36, 95% CI 0.23-172.73; year 3: OR 3.94, 85% CI 1.46-10.69; year 5: OR 5.34, 95% CI 1.87-15.29).
Conclusion: This systematic review and meta-analysis suggests that patients compliant with EVAR surveillance programmes may have an increased re-intervention rate but do not appear to have better survival rates than non-compliant patients.
Keywords: Abdominal aortic aneurysm; Endovascular procedures; Epidemiology; Meta-analysis; Review; Stents.
Copyright © 2017 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
I.L. has received research grants from Medtronic Endovascular and Endologix. K.S. is a consultant advisor for Endologix. M.M.T. is the Chief Medical Officer for Endologix.
Figures
Comment in
-
Commentary on "The Implications of Non-compliance for Endovascular Aneurysm Repair (EVAR)".Eur J Vasc Endovasc Surg. 2018 Apr;55(4):503. doi: 10.1016/j.ejvs.2018.01.011. Epub 2018 Feb 23. Eur J Vasc Endovasc Surg. 2018. PMID: 29478912 No abstract available.
References
-
- Reise JA, Sheldon H, Earnshaw J, Naylor AR, Dick F, Powell JT, et al. Patient preference for surgical method of abdominal aortic aneurysm repair: postal survey. Eur J Vasc Endovasc Surg. 2010;39:55–61. - PubMed
-
- Nordon IM, Karthikesalingam A, Hinchliffe RJ, Holt PJ, Loftus IM, Thompson MM. Secondary interventions following endovascular aneurysm repair (EVAR) and the enduring value of graft surveillance. Eur J Vasc Endovasc Surg. 2010;39:547–54. - PubMed
-
- Karthikesalingam A, Holt PJE, Hinchliffe RJ, Nordon IM, Loftus IM, Thompson MM. Risk of reintervention after endovascular aortic aneurysm repair. Br J Surg. 2010;97:657–63. - PubMed
-
- Chaikof EL, Brewster DC, Dalman RL, Makaroun MS, Illig KA, Sicard GA, et al. SVS practice guidelines for the care of patients with an abdominal aortic aneurysm: executive summary. J Vasc Surg. 2009;50:880–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
