

Clinical Profile of Patients Admitted with Hyponatremia in the Medical Intensive Care Unit
- PMID: 29307961
- PMCID: PMC5752789
- DOI: 10.4103/ijccm.IJCCM_257_17
Clinical Profile of Patients Admitted with Hyponatremia in the Medical Intensive Care Unit
Abstract
Background and aims: Hyponatremia is the predominant electrolyte abnormality with an incidence rate of approximately 22%. It is the leading cause of morbidity and mortality with scarce data in Indian intensive care settings. The aim of this study is to evaluate the clinical features and etiology of hyponatremia in patients admitted to an Intensive Care Unit (ICU) of a tertiary care hospital.
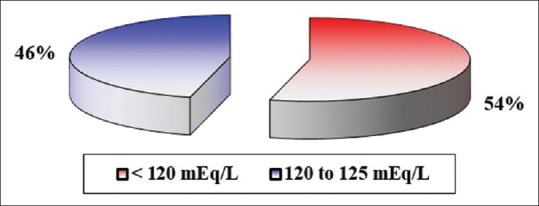
Materials and methods: A 1-year prospective cross-sectional observational study was conducted, including 100 adult patients with moderate-to-severe hyponatremia admitted to the Medical ICU. Patients underwent investigations such as serum creatinine, blood urea nitrogen, serum osmolality, serum sodium, urine sodium, and urine osmolality, sputum culture, cerebrospinal fluid analysis, and neuroimaging. Data were analyzed using independent sample t-test, Chi-square test, and Fisher's exact test.
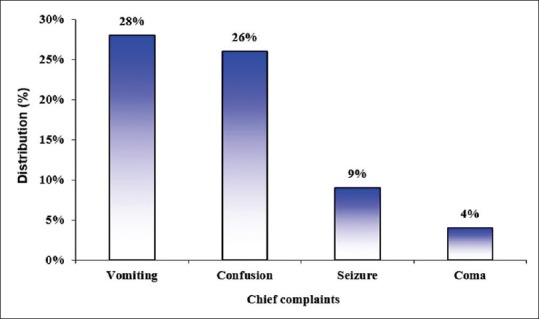
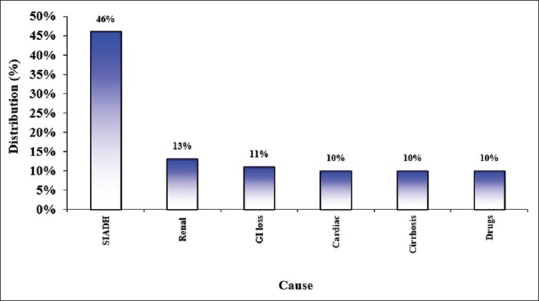
Results: Vomiting (28) followed by confusion (26) was the most common complaint. Syndrome of inappropriate antidiuretic hormone secretion (SIADH) (46) was the most common etiology for hyponatremia, and euvolemic hypoosmolar hyponatremia (50) was the most common type of hyponatremia. Confusion was significantly high in patients with severe hyponatremia as compared to patients with moderate hyponatremia (22 vs. 4, P < 0.001). In majority of the patients (46), SIADH was the main cause of euvolemic type of hyponatremia (P < 0.001). Increased urine sodium levels were observed in patients with SIADH (46), renal dysfunction (12), and drug-induced etiology (8, P < 0.001).
Conclusion: Patients with hyponatremia secondary to an infectious cause should be meticulously screened for tuberculosis. The timely and effective treatment of hyponatremia is determined by the effective understanding of pathophysiology and associated risk factors of hyponatremia.
Keywords: Hyponatremia; moderate and severe hyponatremia; serum sodium; syndrome of inappropriate antidiuretic hormone secretion; tuberculosis.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Fried LF, Palevsky PM. Hyponatremia and hypernatremia. Med Clin North Am. 1997;81:585–609. - PubMed
-
- Fall PJ. Hyponatremia and hypernatremia. A systematic approach to causes and their correction. Postgrad Med. 2000;107:75–82. - PubMed
-
- Freda BJ, Davidson MB, Hall PM. Evaluation of hyponatremia: A little physiology goes a long way. Cleve Clin J Med. 2004;71:639–50. - PubMed
-
- Han DS, Cho BS. Therapeutic approach to hyponatremia. Nephron. 2002;92(Suppl 1):9–13. - PubMed
-
- Pham PC, Pham PM, Pham PT. Vasopressin excess and hyponatremia. Am J Kidney Dis. 2006;47:727–37. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources