

Nomogram based on tumor-associated neutrophil-to-lymphocyte ratio to predict survival of patients with gastric neuroendocrine neoplasms
- PMID: 29307997
- PMCID: PMC5743508
- DOI: 10.3748/wjg.v23.i47.8376
Nomogram based on tumor-associated neutrophil-to-lymphocyte ratio to predict survival of patients with gastric neuroendocrine neoplasms
Abstract
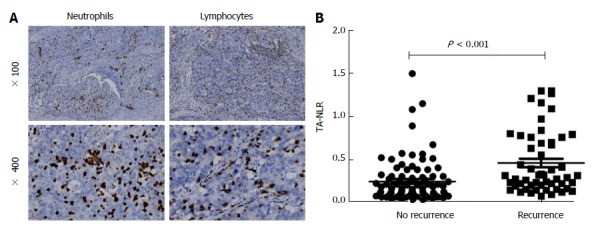
Aim: To assess the predictive value of the tumor-associated neutrophil-to-lymphocyte ratio in terms of the clinical outcomes of patients with gastric neuroendocrine neoplasms after radical surgery.
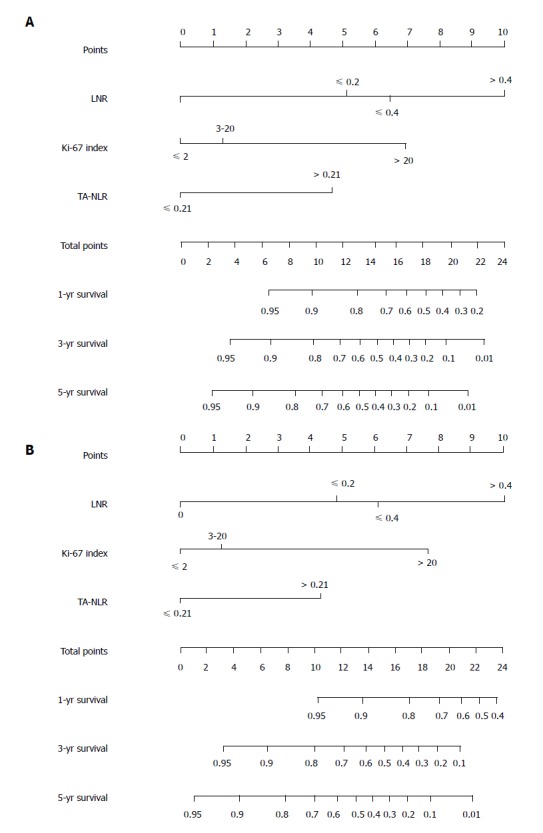
Methods: Data were retrospectively collected from 142 patients who were diagnosed with gastric neuroendocrine neoplasms and who underwent radical gastrectomy at our department from March 2006 to March 2015. These data were retrospectively analyzed, and a receiver operating characteristic curve analysis was used to identify the optimal value of the tumor-associated neutrophil-to-lymphocyte ratio. Univariate and multivariate survival analyses were used to identify prognostic factors. A nomogram was then applied to predict clinical outcomes after surgery.
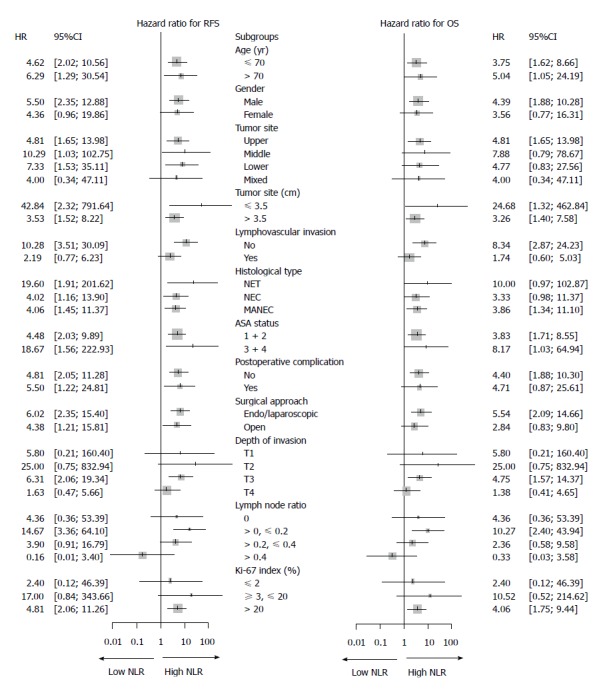
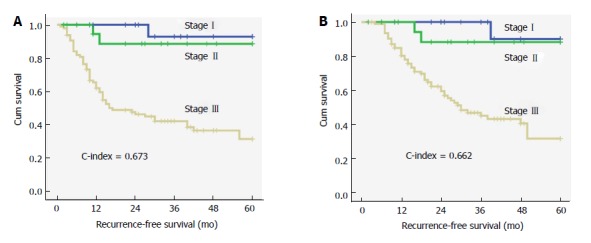
Results: The tumor-associated neutrophil-to-lymphocyte ratio was significantly associated with tumor recurrence, especially with liver metastasis and lymph node metastasis (P < 0.05 for both), but not with clinical characteristics (P > 0.05 for all). A multivariate Cox regression analysis identified the tumor-associated neutrophil-to-lymphocyte ratio as an independent prognostic factor for recurrence-free survival and overall survival (P < 0.05 for both). The concordance index of the nomograms, which included the tumor-associated neutrophil-to-lymphocyte ratio, Ki-67 index, and lymph node ratio, was 0.788 (0.759) for recurrence-free survival (overall survival) and was higher than the concordance index of the traditional TNM staging system [0.672 (0.663)].
Conclusion: The tumor-associated neutrophil-to-lymphocyte ratio is an independent prognostic factor in patients with gastric neuroendocrine neoplasms. Nomograms that include the tumor-associated neutrophil-to-lymphocyte ratio, Ki-67 index, and lymph node ratio have a superior ability to predict clinical outcomes of postoperative patients.
Keywords: Gastric neuroendocrine neoplasms; Prognosis; Tumor recurrence; Tumor-associated neutrophil-to-lymphocyte ratio.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that there are no conflicts of interest associated with the publication of this manuscript.
Figures
References
-
- Burkitt MD, Pritchard DM. Review article: Pathogenesis and management of gastric carcinoid tumours. Aliment Pharmacol Ther. 2006;24:1305–1320. - PubMed
-
- Niederle MB, Hackl M, Kaserer K, Niederle B. Gastroenteropancreatic neuroendocrine tumours: the current incidence and staging based on the WHO and European Neuroendocrine Tumour Society classification: an analysis based on prospectively collected parameters. Endocr Relat Cancer. 2010;17:909–918. - PubMed
-
- Klöppel G, Perren A, Heitz PU. The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification. Ann N Y Acad Sci. 2004;1014:13–27. - PubMed
-
- Bosman FT, Carneiro F, Theise ND. Nomenclature and classification of neuroendocrine neoplasms of digestive system. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC Press; 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
