

Invasive Obstetric Procedures and Cesarean Sections in Women With Known Herpes Simplex Virus Status During Pregnancy
- PMID: 29308404
- PMCID: PMC5751035
- DOI: 10.1093/ofid/ofx248
Invasive Obstetric Procedures and Cesarean Sections in Women With Known Herpes Simplex Virus Status During Pregnancy
Abstract
Background: Neonatal herpes is a potentially devastating infection that results from acquisition of herpes simplex virus (HSV) type 1 or 2 from the maternal genital tract at the time of vaginal delivery. Current guidelines recommend (1) cesarean delivery if maternal genital HSV lesions are present at the time of labor and (2) antiviral suppressive therapy for women with known genital herpes to decrease HSV shedding from the genital tract at the time of vaginal delivery. However, most neonatal infections occur in infants born to women without a history of genital HSV, making current prevention efforts ineffective for this group. Although routine serologic HSV testing of women during pregnancy could identify women at higher risk of intrapartum viral shedding, it is uncertain how this knowledge might impact intrapartum management, and a potential concern is a higher rate of cesarean sections among women known to be HSV-2 seropositive.
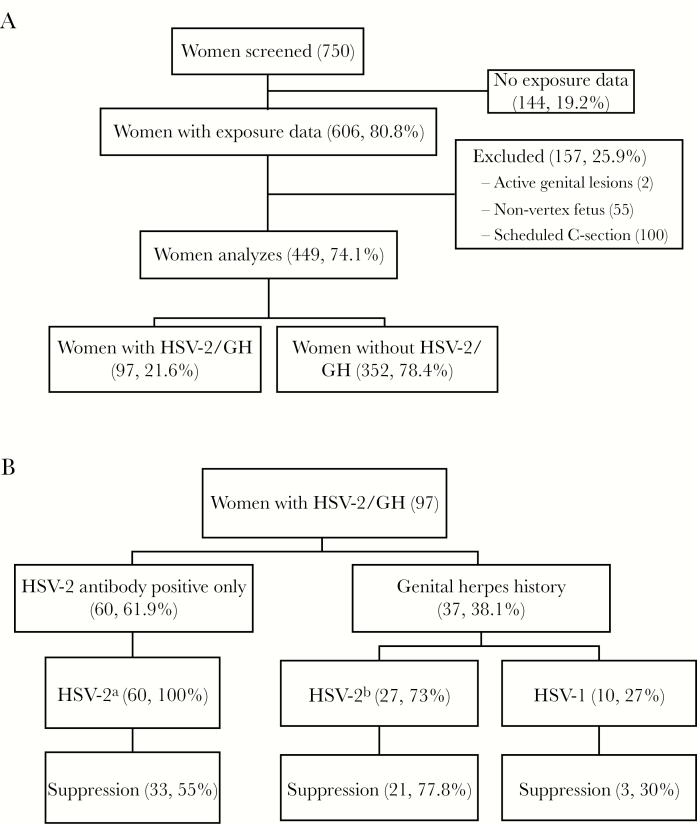
Methods: To assess the effects of prenatal HSV-2 antibody testing, history of genital herpes, and use of suppressive antiviral medication on the intrapartum management of women, we investigated the frequency of invasive obstetric procedures and cesarean deliveries. We conducted a retrospective cohort study of pregnant women delivering at the University of Washington Medical center in Seattle, Washington. We defined the exposure of interest as HSV-2 antibody positivity or known history of genital herpes noted in prenatal records. The primary outcome was intrapartum procedures including fetal scalp electrode, artificial rupture of membranes, intrauterine pressure catheter, or operative vaginal delivery (vacuum or forceps). The secondary outcome was incidence of cesarean birth. Univariate and multivariable logistic regressions were performed.
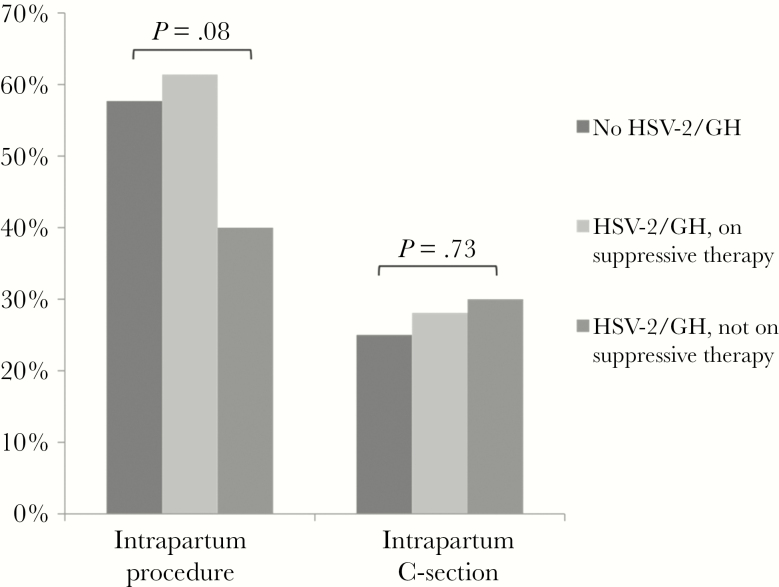
Results: From a total of 449 women included in the analysis, 97 (21.6%) were HSV-2 seropositive or had a history of genital herpes (HSV-2/GH). Herpes simplex virus-2/GH women not using suppressive antiviral therapy were less likely to undergo intrapartum procedures than women without HSV-2/GH (odds ratio [OR], 0.49; 95% confidence interval [CI], 0.25-0.95; P = .036), but this relationship was attenuated after adjustment for potential confounders (adjusted OR, 0.69; 95% CI, 0.34-1.41; P = .31). There was no difference in intrapartum procedures for women on suppressive therapy versus women without HSV-2/GH (OR, 1.17; 95% CI, 0.66-2.07; P = .60). Similar proportions of cesarean sections were performed within each group of women: 25% without history of HSV-2/GH, 30% on suppressive treatment, and 28.1% without suppressive treatment (global, P = .73).
Conclusions: In this single-site study, provider awareness of genital herpes infection either by HSV serotesting or history was associated with fewer invasive obstetric procedures shown to be associated with neonatal herpes, but it was not associated with an increased rate of cesarean birth.
Keywords: cesarean section; genital herpes; herpes simplex virus-2; pregnancy; suppressive therapy.
Figures
Similar articles
-
Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant.JAMA. 2003 Jan 8;289(2):203-9. doi: 10.1001/jama.289.2.203. JAMA. 2003. PMID: 12517231
-
Genital herpes complicating pregnancy.Obstet Gynecol. 2005 Oct;106(4):845-56. doi: 10.1097/01.AOG.0000180779.35572.3a. Obstet Gynecol. 2005. PMID: 16199646 Review.
-
Cost-effectiveness of herpes simplex virus type 2 serologic testing and antiviral therapy in pregnancy.Am J Obstet Gynecol. 2004 Dec;191(6):2074-84. doi: 10.1016/j.ajog.2004.05.034. Am J Obstet Gynecol. 2004. PMID: 15592294
-
Preventing herpes simplex virus transmission to the neonate.Herpes. 2004 Aug;11 Suppl 3:175A-186A. Herpes. 2004. PMID: 15319088 Review.
-
Herpes simplex virus type 2 and risk of intrapartum human immunodeficiency virus transmission.Obstet Gynecol. 2007 Feb;109(2 Pt 1):403-9. doi: 10.1097/01.AOG.0000251511.27725.5c. Obstet Gynecol. 2007. PMID: 17267842
Cited by
-
Healthcare resource utilisation pattern and costs associated with herpes simplex virus diagnosis and management: a systematic review.BMJ Open. 2022 Jan 4;12(1):e049618. doi: 10.1136/bmjopen-2021-049618. BMJ Open. 2022. PMID: 34983754 Free PMC article.
References
-
- Brown ZA, Wald A, Morrow RA et al. . Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant. JAMA 2003; 289:203–9. - PubMed
-
- Mark KE, Kim HN, Wald A et al. . Targeted prenatal herpes simplex virus testing: can we identify women at risk of transmission to the neonate?Am J Obstet Gynecol 2006; 194:408–14. - PubMed
-
- Whitley R, Davis EA, Suppapanya N. Incidence of neonatal herpes simplex virus infections in a managed-care population. Sex Transm Dis 2007; 34:704–8. - PubMed
-
- Morris SR, Bauer HM, Samuel MC et al. . Neonatal herpes morbidity and mortality in California, 1995–2003. Sex Transm Dis 2008; 35:14–8. - PubMed
-
- Handel S, Klingler EJ, Washburn K et al. . Population-based surveillance for neonatal herpes in New York City, April 2006-September 2010. Sex Transm Dis 2011; 38:705–11. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
