

Haemoglobin glycation index and risk for diabetes-related complications in the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial
- PMID: 29308539
- PMCID: PMC6448976
- DOI: 10.1007/s00125-017-4539-1
Haemoglobin glycation index and risk for diabetes-related complications in the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial
Abstract
Aims/hypothesis: Previous studies have suggested that the haemoglobin glycation index (HGI) can be used as a predictor of diabetes-related complications in individuals with type 1 and type 2 diabetes. We investigated whether HGI was a predictor of adverse outcomes of intensive glucose lowering and of diabetes-related complications in general, using data from the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial.
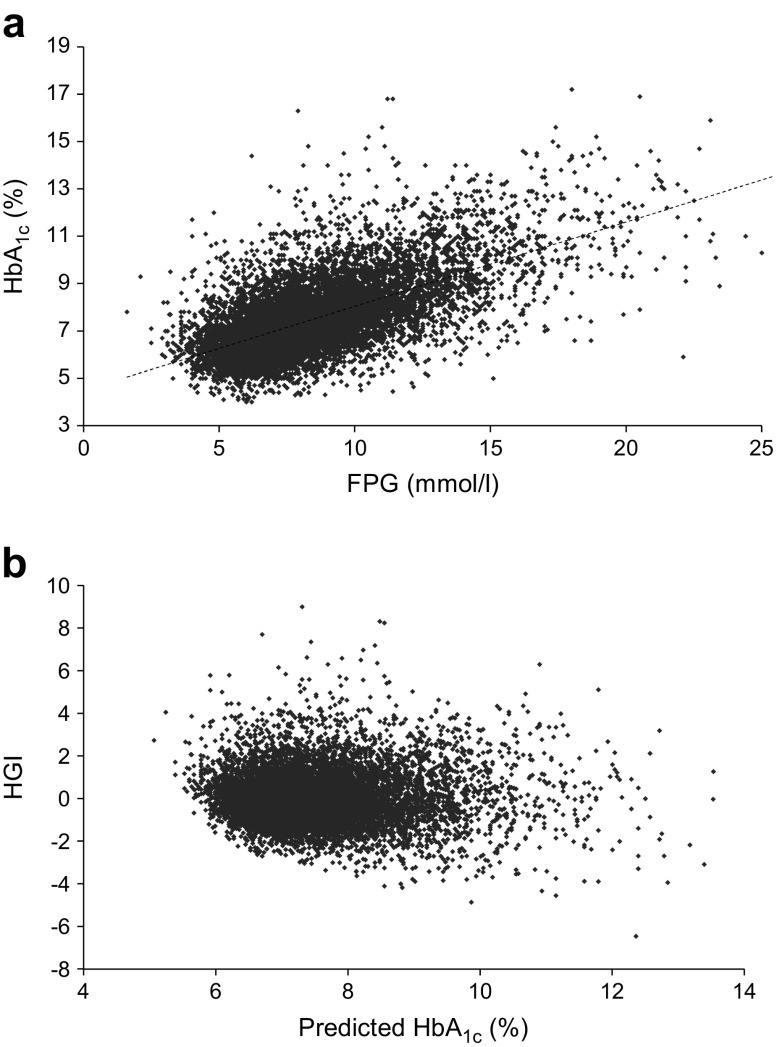
Methods: We studied participants in the ADVANCE trial with data available for baseline HbA1c and fasting plasma glucose (FPG) (n = 11,083). HGI is the difference between observed HbA1c and HbA1c predicted from a simple linear regression of HbA1c on FPG. Using Cox regression, we investigated the association between HGI, both categorised and continuous, and adverse outcomes, considering treatment allocation (intensive or standard glucose control) and compared prediction of HGI and HbA1c.
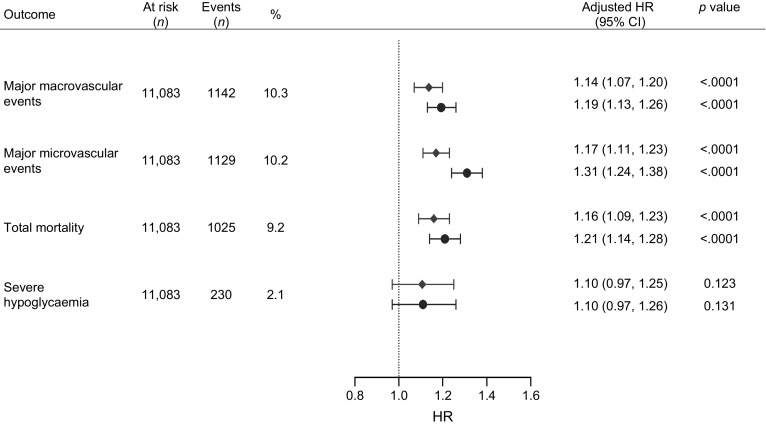
Results: Intensive glucose control lowered mortality risk in individuals with high HGI only (HR 0.74 [95% CI 0.61, 0.91]; p = 0.003), while there was no difference in the effect of intensive treatment on mortality in those with high HbA1c. Irrespective of treatment allocation, every SD increase in HGI was associated with a significant risk increase of 14-17% for macrovascular and microvascular disease and mortality. However, when adjusted for identical covariates, HbA1c was a stronger predictor of these outcomes than HGI.
Conclusions/interpretation: HGI predicts risk for complications in ADVANCE participants, irrespective of treatment allocation, but no better than HbA1c. Individuals with high HGI have a lower risk for mortality when on intensive treatment. Given the discordant results and uncertain relevance beyond HbA1c, clinical use of HGI in type 2 diabetes cannot currently be recommended.
Keywords: (Blood) glucose; Cardiovascular complications; Diabetes mellitus, type 2; HbA1c; Hypoglycaemia; Mortality.
Conflict of interest statement
MW received consulting fees from Amgen. JC received research grants and speaker fees from Servier. MM received personal fees from Novo Nordisk, Sanofi, Eli Lilly, Merck Sharp and Dohme, Abbott, Novartis and AstraZeneca and grant support from Novo Nordisk, Sanofi, Eli Lilly, Merck Sharp and Dohme and Novartis. MEC received consulting fees from Merck, GlaxoSmithKline, Amgen and AstraZeneca and lecture fees from Servier. PH received consulting fees from Servier. GM received lecture fees from Bayer, Boehringer Ingelheim, Daiichi-Sankyo, Medtronic, Novartis, Menarini International, Recordati, Servier and Takeda. SC received fees for serving on advisory boards and lecture fees from Servier. BW received lecture fees from Novartis, Boehringer Ingelheim and Merck Sharpe and Dohme. DEG received lecture fees from Servier and consulting and lecture fees and grant support from Pfizer, AstraZeneca, Novartis and Sanofi-Aventis. JHDV received speaker fees from Novo Nordisk and Senseonics, research support from Abbott, Dexcom, Medtronic, Novo Nordisk, Sanofi and Senseonics, and fees for serving on advisory boards from Merck Sharpe and Dohme, Novo Nordisk, Roche and Sanofi. The remaining author declares that there is no duality of interest associated with their contribution to this manuscript.
Figures
References
-
- ADA (2016) Standards of medical care in diabetes. Available from http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_.... Accessed 1 July 2017
-
- Abraira C, Colwell J, Nuttall F, et al. Cardiovascular events and correlates in the Veterans Affairs Diabetes Feasibility Trial. Veterans Affairs Cooperative Study on Glycemic Control and Complications in Type II Diabetes. Arch Intern Med. 1997;157:181–188. doi: 10.1001/archinte.1997.00440230053007. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
