

Curbing the hepatitis C virus epidemic in Pakistan: the impact of scaling up treatment and prevention for achieving elimination
- PMID: 29309592
- PMCID: PMC5913612
- DOI: 10.1093/ije/dyx270
Curbing the hepatitis C virus epidemic in Pakistan: the impact of scaling up treatment and prevention for achieving elimination
Abstract
Background: The World Health Organization (WHO) has developed a global health strategy to eliminate viral hepatitis. We project the treatment and prevention requirements to achieve the WHO HCV elimination target of reducing HCV incidence by 80% and HCV-related mortality by 65% by 2030 in Pakistan, which has the second largest HCV burden worldwide.
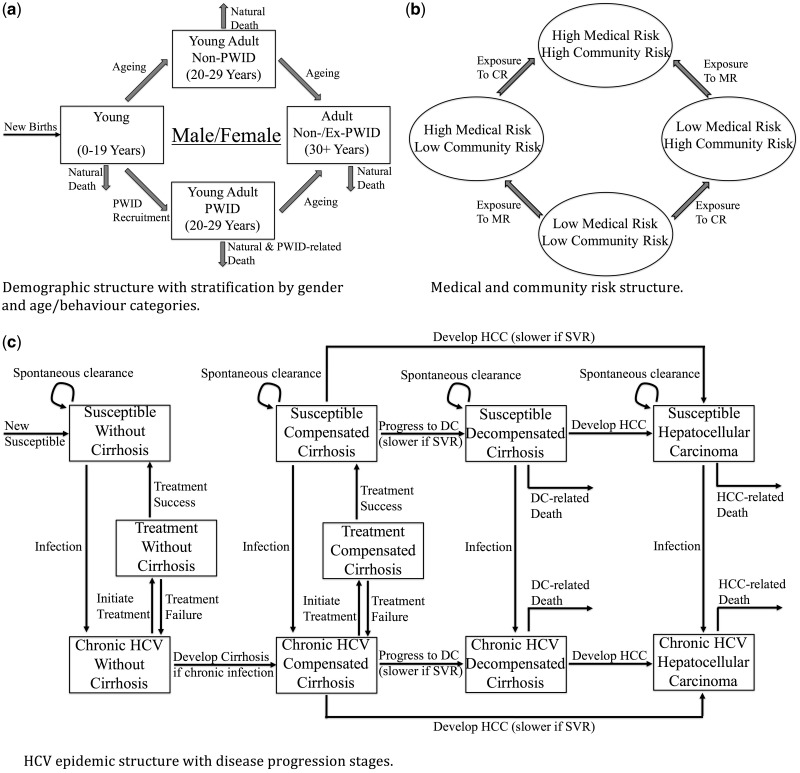
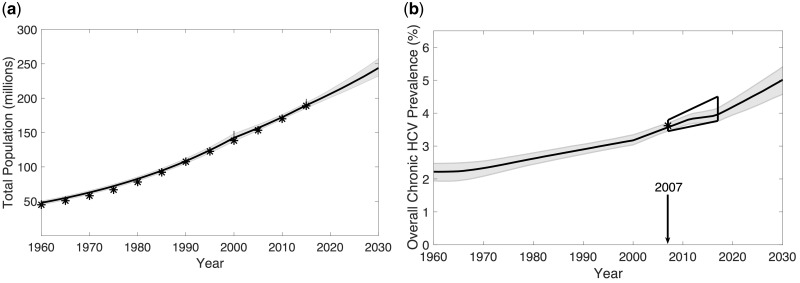
Methods: We developed an HCV transmission model for Pakistan, and calibrated it to epidemiological data from a national survey (2007), surveys among people who inject drugs (PWID), and blood donor data. Current treatment coverage data came from expert opinion and published reports. The model projected the HCV burden, including incidence, prevalence and deaths through 2030, and estimated the impact of varying prevention and direct-acting antiviral (DAA) treatment interventions necessary for achieving the WHO HCV elimination targets.
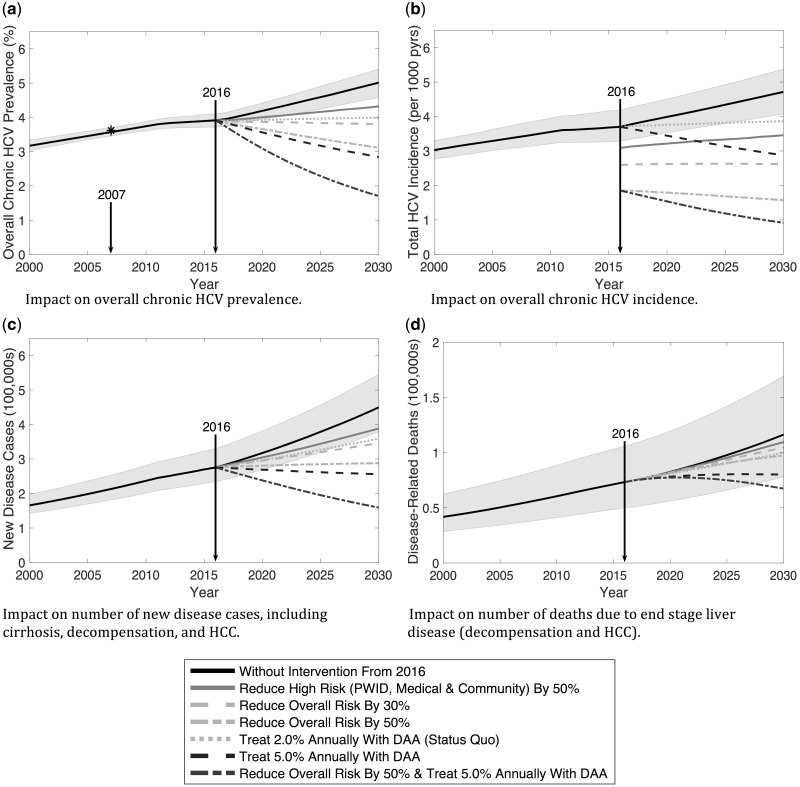
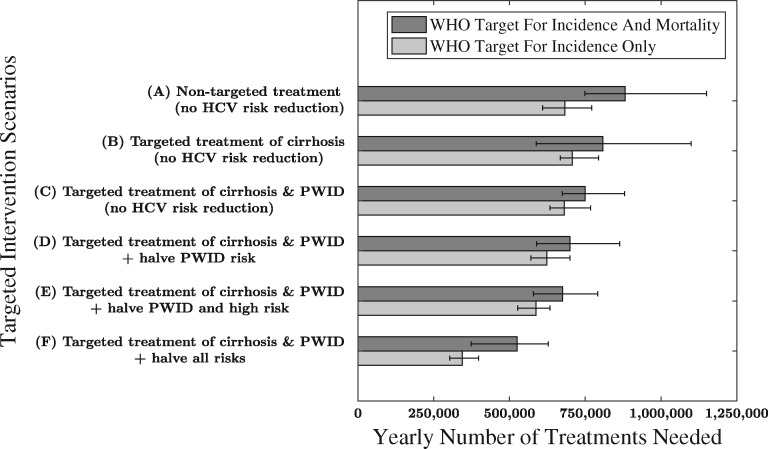
Results: With no further treatment (currently ∼150 000 treated annually) during 2016-30, chronic HCV prevalence will increase from 3.9% to 5.1%, estimated annual incident infections will increase from 700 000 to 1 100 000, and 1 400 000 HCV-associated deaths will occur. To reach the WHO HCV elimination targets by 2030, 880 000 annual DAA treatments are required if prevention is not scaled up and no treatment prioritization occurs. By targeting treatment toward persons with cirrhosis (80% treated annually) and PWIDs (double the treatment rate of non-PWIDs), the required annual treatment number decreases to 750 000. If prevention activities also halve transmission risk, this treatment number reduces to 525 000 annually.
Conclusions: Substantial HCV prevention and treatment interventions are required to reach the WHO HCV elimination targets in Pakistan, without which Pakistan's HCV burden will increase markedly.
Figures
Comment in
-
The cost of eliminating hepatitis C in Pakistan.Lancet Glob Health. 2020 Mar;8(3):e323-e324. doi: 10.1016/S2214-109X(20)30036-X. Lancet Glob Health. 2020. PMID: 32087161 No abstract available.
References
-
- Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H.. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014;61(Suppl 1):S45–57. - PubMed
-
- World Health Organization. Global Hepatitis Report, 2017. Geneva: WHO, 2017.
-
- Graham CS, Swan T.. A path to eradication of hepatitis C in low- and middle-income countries. Antiviral Res 2015;119:89–96. - PubMed
-
- World Health Organization. Guidelines for the Screening Care and Treatment of Persons with Chronic Hepatitis C Infection: Updated Version. Geneva: World Health Organization, 2016. - PubMed
-
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016-2021. Towards Ending Viral Hepatitis. Geneva: WHO, 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
