

Obtaining adequate lamina propria for subepithelial fibrosis evaluation in pediatric eosinophilic esophagitis
- PMID: 29309779
- PMCID: PMC5899929
- DOI: 10.1016/j.gie.2017.12.020
Obtaining adequate lamina propria for subepithelial fibrosis evaluation in pediatric eosinophilic esophagitis
Abstract
Background and aims: Subepithelial fibrosis in eosinophilic esophagitis (EoE) can be detected only in esophageal biopsy specimens with adequate amounts of lamina propria (LP). We investigated how often pediatric esophageal biopsy specimens contain adequate LP, and whether esophageal eosinophilia influences the acquisition rates.
Methods: We evaluated 284 esophageal biopsy specimens from 39 patients with EoE, and 87 biopsy specimens from 32 patients without esophageal eosinophilia or other esophageal abnormalities for the presence of adequate LP and fibrosis.
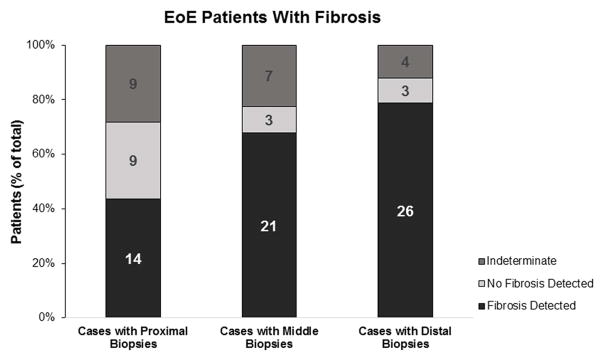
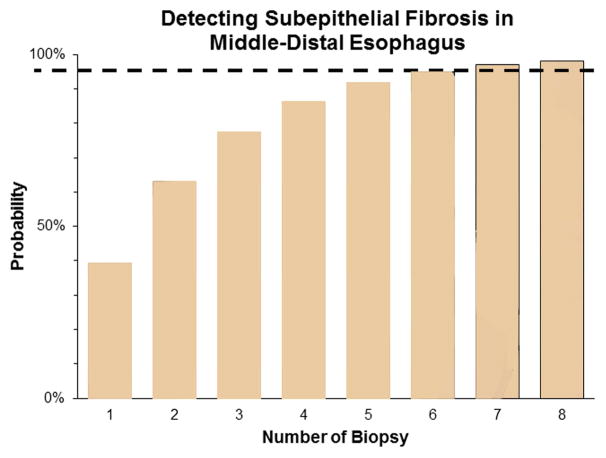
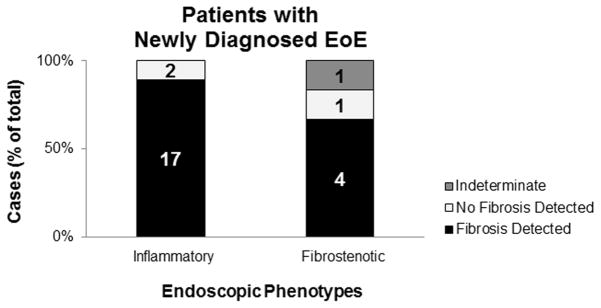
Results: On a per biopsy specimen basis, there was no significant difference in the rate of procuring adequate amounts of LP between patients with EoE and patients without esophageal eosinophilia (43% vs 31%, P = .14). Eighty-five percent of patients with EoE had fibrosis. Fibrosis in patients with EoE was patchy and more likely to be detected in the middle or distal esophagus (odds ratio, 19.93; 95% confidence interval, 4.12-91.52). Among patients with fibrosis, the probability of its detection reached >95% with 7 middle-distal esophageal biopsy specimens. Most children with newly diagnosed EoE already had subepithelial fibrosis despite exhibiting only inflammatory endoscopic features.
Conclusions: Most individual esophageal biopsy specimens in children are inadequate for assessing subepithelial fibrosis, and the rates of procuring adequate LP per biopsy specimen are similar in patients with and without EoE. To reliably detect fibrosis in patients with EoE, at least 7 biopsy specimens should be taken from the middle-distal esophagus. The finding of fibrosis in children with newly diagnosed EoE and only inflammatory endoscopic features suggests that fibrosis can occur early in this disease.
Copyright © 2018 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20. e6. quiz 21–2. - PubMed
-
- Aceves SS. Tissue remodeling in patients with eosinophilic esophagitis: what lies beneath the surface? J Allergy Clin Immunol. 2011;128:1047–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
