

Improvements in osteoporosis testing and care are found following the wide scale implementation of the Ontario Fracture Clinic Screening Program: An interrupted time series analysis
- PMID: 29310418
- PMCID: PMC5728819
- DOI: 10.1097/MD.0000000000009012
Improvements in osteoporosis testing and care are found following the wide scale implementation of the Ontario Fracture Clinic Screening Program: An interrupted time series analysis
Abstract
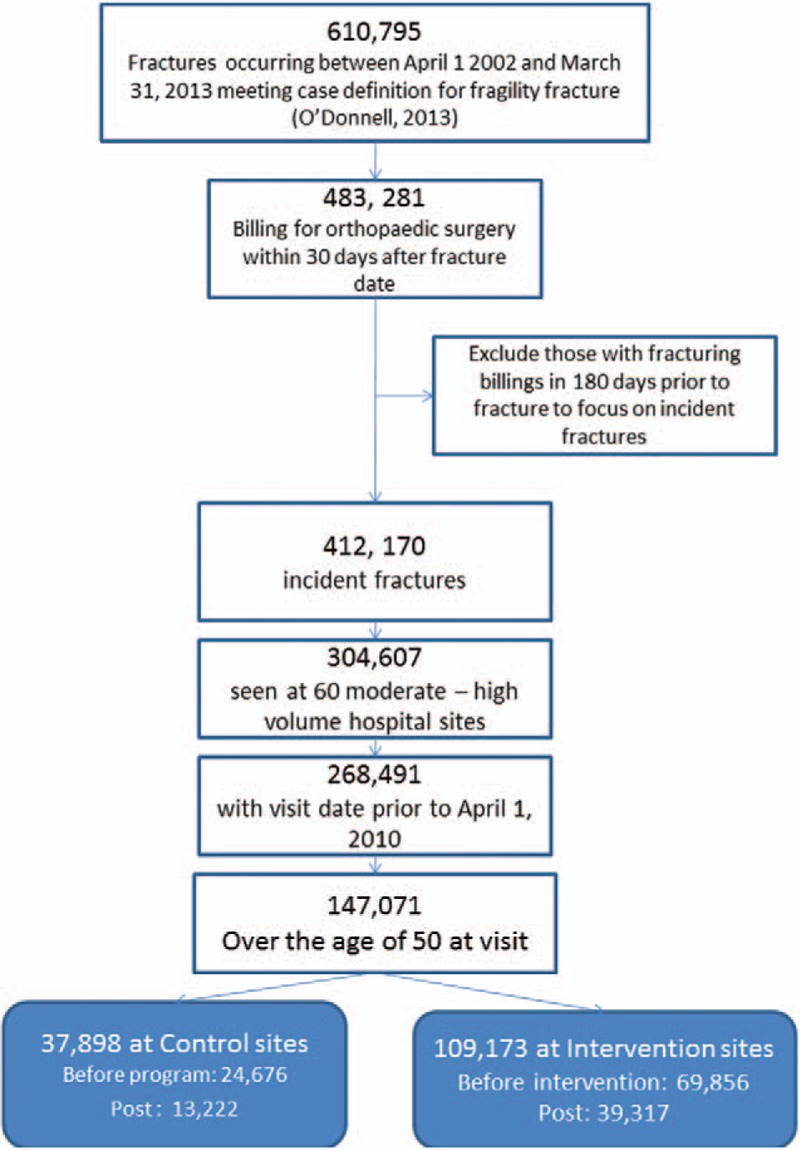
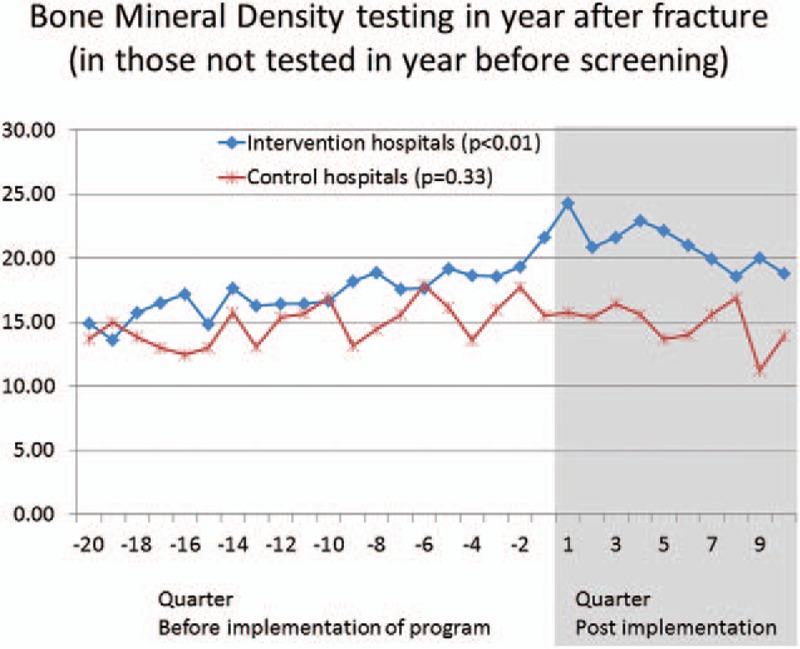
We evaluated a system-wide impact of a health intervention to improve treatment of osteoporosis after a fragility fracture. The intervention consisted of assigning a screening coordinator to selected fracture clinics to identify, educate, and follow up with fragility fracture patients and inform their physicians of the need to evaluate bone health. Thirty-seven hospitals in the province of Ontario (Canada) were assigned a screening coordinator. Twenty-three similar hospitals were control sites. All hospitals had orthopedic services and handled moderate-to-higher volumes of fracture patients. Administrative health data were used to evaluate the impact of the intervention.Fragility fracture patients (≥50 years; hip, humerus, forearm, spine, or pelvis fracture) were identified from administrative health records. Cases were fractures treated at 1 of the 37 hospitals assigned a coordinator. Controls were the same types of fractures at the control sites. Data were assembled for 20 quarters before and 10 quarters after the implementation (from January 2002 to March 2010). To test for a shift in trends, we employed an interrupted time series analysis-a study design used to evaluate the longitudinal effects of interventions, through regression modelling. The primary outcome measure was bone mineral density (BMD) testing. Osteoporosis medication initiation and persistence rates were secondary outcomes in a subset of patients ≥66 years of age.A total of 147,071 patients were used in the analysis. BMD testing rates increased from 17.0% pre-intervention to 20.9% post-intervention at intervention sites (P < .01) compared with no change at control sites (14.9% and 14.9%, P = .33). Medication initiation improved significantly at intervention sites (21.6-23.97%; P = .02) but not at control sites (17.5-18.5%; P = .27). Persistence with bisphosphonates decreased at all sites, from 59.9% to 56.4% at intervention sites (P = .02) and more so from 62.3% to 54.2% at control sites (P < .01) using 50% proportion of days covered (PDC 50).Significant improvements in BMD testing and treatment initiation were observed after the initiation of a coordinator-based screening program to improve osteoporosis management following fragility fracture.
Conflict of interest statement
The rest of the authors declare no conflict of interest.
Figures
References
-
- Colón-Emeric C, Kuchibhatla M, Pieper C, et al. The contribution of hip fracture to risk of subsequent fractures: data from two longitudinal studies. Osteoporos Int 2003;14:879–83. - PubMed
-
- Haentjens P, Autier P, Collins J, et al. Colles fracture, spine fracture, and subsequent risk of hip fracture in men and women. A meta-analysis. J Bone Joint Surg Am 2003;85-A:1936–43. - PubMed
-
- Johnell O, Kanis JA, Odén A, et al. Fracture risk following an osteoporotic fracture. Osteoporos Int 2004;15:175–9. - PubMed
-
- Klotzbuecher CM, Ross PD, Landsman PB, et al. Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 2000;15:721–39. - PubMed
-
- Bliuc D, Nguyen ND, Milch VE, et al. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA 2009;301:513–21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
