

Does presence of metabolic syndrome impact anxiety and depressive disorder screening results in middle aged and elderly individuals? A population based study
- PMID: 29310620
- PMCID: PMC5759833
- DOI: 10.1186/s12888-017-1576-8
Does presence of metabolic syndrome impact anxiety and depressive disorder screening results in middle aged and elderly individuals? A population based study
Abstract
Background: Depressive and anxiety disorders are common in primary care setting but often remain undiagnosed. Metabolic syndrome (MetS) is also prevalent in the general population and can impair recognition of common mental disorders due to significant co-morbidity and overlap with psychiatric symptoms included in self-reported depression/anxiety screening tools. We investigated if MetS has an impact on the accuracy of current major depressive disorder (MDD) and generalized anxiety disorder (GAD) screening results using the Hospital Anxiety and Depression scale (HADS).
Methods: A total of 1115 (562 men; mean age 62.0 ± 9.6 years) individuals of 45+ years of age were randomly selected from the general population and evaluated for current MetS; depressive and anxiety symptoms (HADS); and current MDD and GAD (Mini International Neuropsychiatric Interview [MINI]).
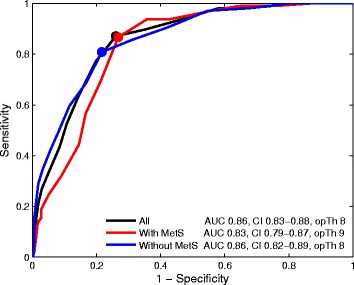
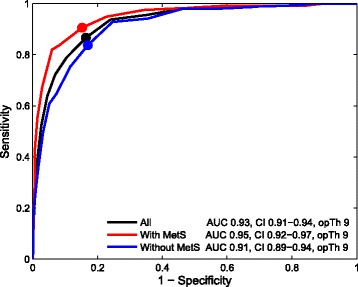
Results: The MetS was diagnosed in 34.4% of the study participants. Current MDD and GAD were more common in individuals with MetS relative to individuals without MetS (25.3% vs 14.2%, respectively, p < 0.001; and 30.2% vs 20.9%, respectively, p < 0.001). The ROC analyses demonstrated that optimal thresholds of the HADS-Depression subscale for current MDE were ≥9 in individuals with MetS (sensitivity = 87%, specificity = 73% and PPV = 52%) and ≥8 in individuals without MetS (sensitivity = 81%, specificity = 78% and PPV = 38%). At threshold of ≥9 the HADS-Anxiety subscale demonstrated optimal psychometric properties for current GAD screening in individuals with MetS (sensitivity = 91%, specificity = 85% and PPV = 72%) and without MetS (sensitivity = 84%, specificity = 83% and PPV = 56%).
Conclusions: The HADS is a reliable screening tool for current MDE and GAD in middle aged and elderly population with and without MetS. Optimal thresholds of the HADS-Depression subscale for current MDD is ≥9 for individuals with MetS and ≥8 - without MetS. Optimal threshold of the HADS-Anxiety subscale is ≥9 for current GAD in individuals with and without MetS. The presence of MetS should be considered when interpreting depression screening results.
Keywords: Depressive disorder; General anxiety disorder; Hospital anxiety and depression scale; Metabolic syndrome; Mini international neuropsychiatric interview; Screening.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol and informed consent procedure were approved by the Regional Bioethics Committee at the Lithuanian University of Health Sciences, Kaunas, Lithuania (2003–01-21 No. 6B/2003). The investigation was carried out in accordance with the Declaration of Helsinki. Each participant gave written informed consent prior to all study procedures.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51(1):8–19. - PubMed
-
- Wittchen HU, Kessler RC, Beesdo K, Krause P, Hofler M, Hoyer J. Generalized anxiety and depression in primary care: prevalence, recognition, and management. The Journal of clinical psychiatry. 2002;63(Suppl 8):24–34. - PubMed
-
- Kroenke K, Spitzer RL, Williams JB, Monahan PO, Lowe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–325. - PubMed
-
- Combs H, Markman J. Anxiety disorders in primary care. The Medical clinics of North America. 2014;98(5):1007–1023. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
