

Iatrogenic Creutzfeldt-Jakob disease with Amyloid-β pathology: an international study
- PMID: 29310723
- PMCID: PMC5759292
- DOI: 10.1186/s40478-017-0503-z
Iatrogenic Creutzfeldt-Jakob disease with Amyloid-β pathology: an international study
Abstract
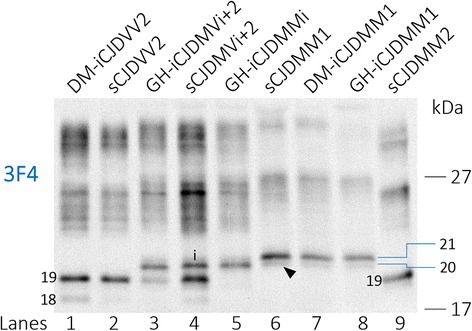
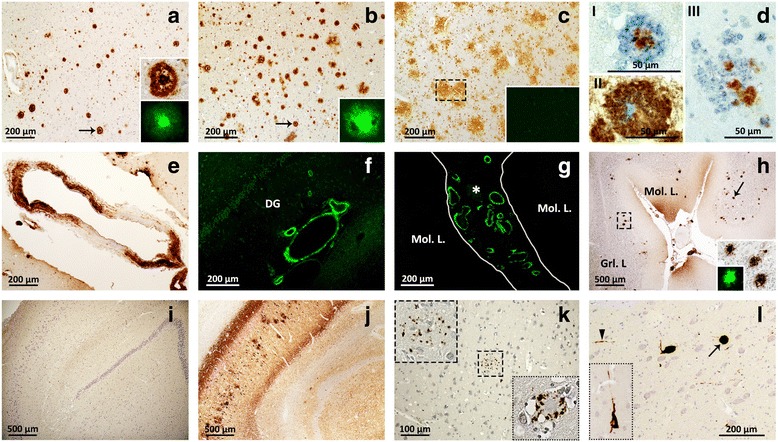
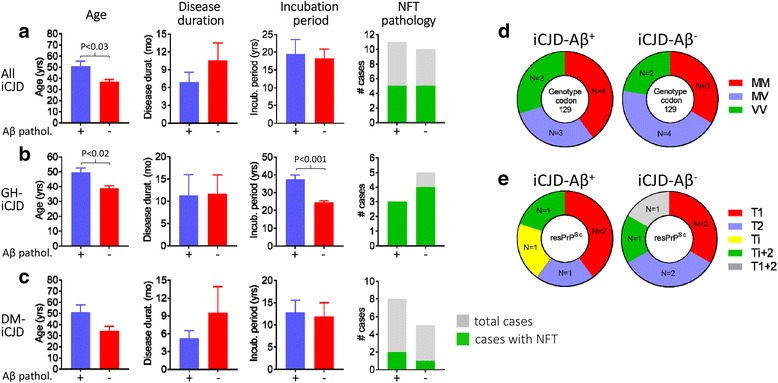
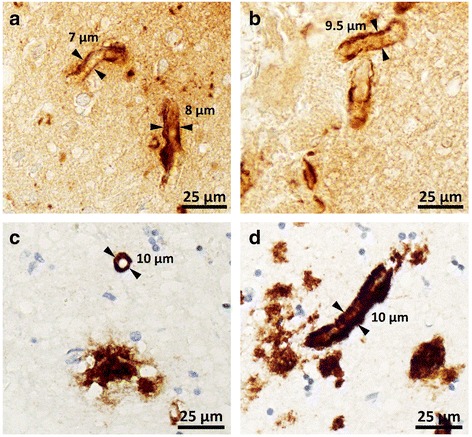
The presence of pathology related to the deposition of amyloid-β (Aβ) has been recently reported in iatrogenic Creutzfeldt-Jakob disease (iCJD) acquired from inoculation of growth hormone (GH) extracted from human cadaveric pituitary gland or use of cadaveric dura mater (DM) grafts.To investigate this phenomenon further, a cohort of 27 iCJD cases - 21 with adequate number of histopathological sections - originating from Australia, France, Italy, and the Unites States, were examined by immunohistochemistry, amyloid staining, and Western blot analysis of the scrapie prion protein (PrPSc), and compared with age-group matched cases of sporadic CJD (sCJD), Alzheimer disease (AD) or free of neurodegenerative diseases (non-ND).Cases of iCJD and sCJD shared similar profiles of proteinase K-resistant PrPSc with the exception of iCJD harboring the "MMi" phenotype. Cerebral amyloid angiopathy (CAA), either associated with, or free of, Thioflavin S-positive amyloid core plaques (CP), was observed in 52% of 21 cases of iCJD, which comprised 37.5% and 61.5% of the cases of GH- and DM-iCJD, respectively. If only cases younger than 54 years were considered, Aβ pathology affected 41%, 2% and 0% of iCJD, sCJD and non-ND, respectively. Despite the patients' younger age CAA was more severe in iCJD than sCJD, while Aβ diffuse plaques, in absence of Aβ CP, populated one third of sCJD. Aβ pathology was by far most severe in AD. Tau pathology was scanty in iCJD and sCJD.In conclusion, (i) despite the divergences in the use of cadaveric GH and DM products, our cases combined with previous studies showed remarkably similar iCJD and Aβ phenotypes indicating that the occurrence of Aβ pathology in iCJD is a widespread phenomenon, (ii) CAA emerges as the hallmark of the Aβ phenotype in iCJD since it is observed in nearly 90% of all iCJD with Aβ pathology reported to date including ours, and it is shared by GH- and DM-iCJD, (iii) although the contributions to Aβ pathology of other factors, including GH deficiency, cannot be discounted, our findings increase the mounting evidence that this pathology is acquired by a mechanism resembling that of prion diseases.
Keywords: Amyloid-β; Cerebral amyloid angiopathy; Pathology; Thioflavin S; iCJD.
Conflict of interest statement
Ethics approval and consent to participate
All patient protocols were approved by the Institutional Review Boards of the University Hospitals Case Medical Center of Cleveland (# 05–14-09). The Australian National CJD Registry has ethical approval for its surveillance operations from The University of Melbourne Human Research Ethics Committee (#1341074.4). In all cases, according to the French regulation, the next of kin provided informed, signed consent in the name of the patient to permit an autopsy and neuropathological investigation. The national computerized registry of objection to autopsy was systematically consulted.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
